Blog
Nov 24, 2025
Why RPA Fails in Home Health?

Arvind Sarin

There is a reason your IT team hates your current automation tools.
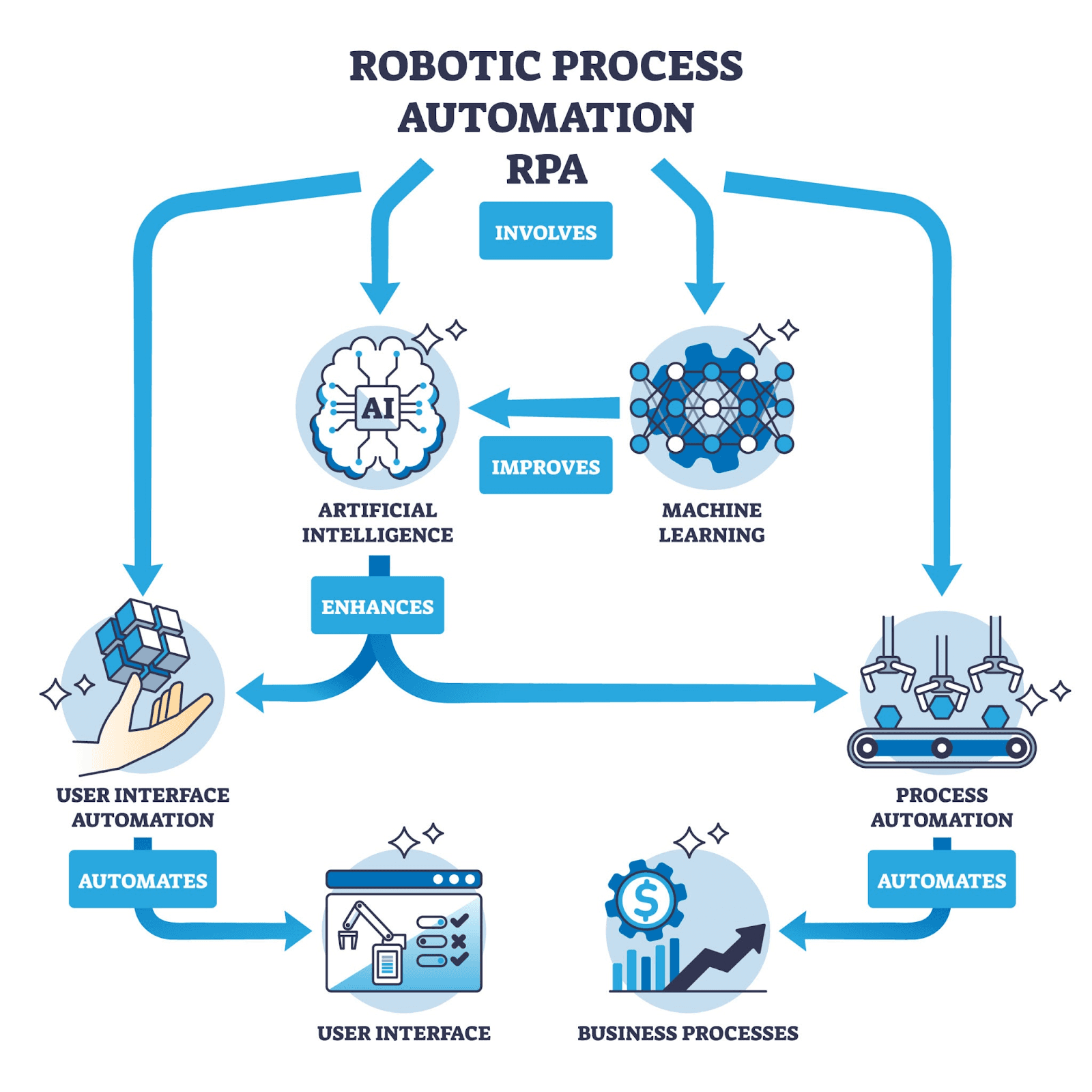
Most home health agencies that claim to use AI are actually using RPA or Robotic Process Automation. Under the hood these are rigid scripts built on specific rules. They rely on CSS Selectors and DOM elements.
The bot is programmed to find the button with a specific ID tag and click it.
This works perfectly in a static environment like manufacturing lines or assembly robots where nothing changes.
But software is not static.
EMRs like WellSky and Homecare Homebase are living platforms. They push updates every month. They change their code. They alter their UI layers. They rebrand. They merge with other companies and rebuild their entire interface.
When a developer at your EMR vendor changes that button's ID code your bot does not just miss the click. It crashes the entire workflow.
This is brittle automation.
You did not buy a digital worker. You bought a script that requires constant surgical maintenance.
The Technical Debt of a "Pixel Perfect" Solution
Here is what actually happens when your RPA bot encounters a software update.
Monday sees your intake bot process 47 referrals flawlessly. Your team celebrates. You finally have time to focus on quality and growth instead of data entry.
Tuesday morning arrives and WellSky pushes a routine interface update. The "Submit" button moves 40 pixels to the right. Its CSS class name changes from btn-primary-submit to btn-submit-primary.
Tuesday afternoon your bot attempts to process an urgent hospital discharge referral. It searches for btn-primary-submit. It cannot find it. It throws an error. It stops.
What happens next is a cascade of failure.
Your intake coordinator receives an error notification. She tries to manually restart the bot. It fails again. She calls your IT vendor. They are closed until tomorrow. She emails them. She opens a support ticket. She manually processes the referral herself.
Meanwhile, 11 other referrals are sitting in the queue. Your response time goes from 45 minutes to 6 hours. The discharge planner who sent that urgent referral calls your competitor instead.
Wednesday brings a response from your vendor. They need to "patch the script." They scheduled a maintenance window for Friday. They bill you $850 for developer time.
Friday sees the patch deployed. The bot works again. Until the next update.
This is not automation. This is a technical debt dressed up as innovation.
The Structured Data Fallacy
The second failure point of traditional RPA is the assumption of structure.
RPA thrives on structured data. It needs spreadsheets and database rows and clean CSVs. It follows a linear logic path. If Column A equals Medicare then populate Field B with value C.
But 80% of healthcare data is unstructured.
Referrals arrive as flat PDFs scanned by a hospital fax machine from 1997. No metadata. No tags. No standardization.
Discharge summaries contain handwritten physician notes in the margins. Written in three different pens by four different people during a 12-hour shift.
Prior authorization forms arrive rotated 90 degrees. Upside down. With coffee stains obscuring the patient's date of birth.
Insurance cards are photographed with an iPhone under fluorescent lighting. Half the text is in shadow. The other half is washed out by glare.
To a standard RPA bot a rotated PDF is unreadable.
It cannot be reasoned that the document needs to be flipped. It cannot infer that the smudged number is probably a 6 instead of an 8 based on context. It simply throws an exception error and dumps the work back onto your human intake coordinators.
If your automation tool only works when the input is perfect it is not solving your problem. It is cherry picking the easy work and leaving you with the hard stuff.
It Is Not the License Fee
Most agencies focus on the wrong cost metric when evaluating automation.
They compare vendor pricing. They negotiate annual license fees. They calculate the cost per bot.
But the real cost of brittle automation is not what you pay upfront. It is what you pay for downtime.
Every time your bot breaks you are paying for three things.
1. Developer hours to patch the script Your vendor charges $150 to $300 per hour. A typical EMR interface update requires 4 to 8 hours of rework. Your patch costs $600 to $2,400. Multiply that by 6 to 12 updates per year. You are spending $7,200 to $28,800 annually just keeping your automation functional.
2. Operational delay while the system is down Your bot processes 40 referrals per day. It is down for 3 days waiting for a patch. That is 120 referrals that now require manual processing. Your intake coordinator works 15 hours of overtime at time and a half. You blow your response time SLA with your top three hospital partners.
3. Staff burnout from sudden manual processing of backlogs Your team got used to the bot handling intake. They redeployed their time to quality assurance and relationship building. Now they are suddenly back to manual data entry. Morale tanks. Your best coordinator starts looking at job postings.
Add these three costs together and a single bot failure can cost you $10,000 to $15,000 in real economic impact.
Now multiply that by 6 to 12 failures per year.
You are spending more money maintaining your automation than you saved by implementing it.
The Shift to Probabilistic Agents
The industry is moving away from scripts toward LLMs and LVMs. Large Language Models and Large Vision Models.
This is not a marketing rebrand. It is a fundamental shift in architecture.
RPA is deterministic. It does exactly what it is told. If the instructions do not match the reality it stops. Full stop. No reasoning. No adaptation. Just failure.
Generative AI is probabilistic. It infers intent. It reasons through ambiguity. It adapts to change.
When a Copper Digital agent looks at a screen it is not hunting for a specific CSS ID. It uses computer vision to read the interface semantically.
The agent understands that a green rectangle with the word "Submit" is the submission button. It does not matter if the button moved 40 pixels to the right. It does not matter if the CSS class changed. It does not matter if the button is now blue instead of green.
The agent understands the goal is to submit the form. It is not just trying to click a specific pixel.
If the form layout changes the agent adapts in real time. No patch required. No developer intervention. No downtime.
Computer Vision vs. Code Inspection: A Technical Deep Dive
Here is the technical difference between how RPA and GenAI agents interact with your EMR.
How RPA Sees Your EMR Step 1 Inspect page HTML Step 2 Locate element with ID="submit-button-primary" Step 3 Execute the click function at coordinates 450, 230 Step 4 Wait 2 seconds Step 5 Verify the element with ID="confirmation-message" appears
What happens when the EMR updates The button ID changes to "primary-submit-button". The coordinates shift to 490, 230. The confirmation message now has ID="message-confirmation". Result Script fails at Step 2. Workflow halts. Human intervention required.
How GenAI Agents See Your EMR Step 1 Capture visual screenshot of interface Step 2 Use computer vision to identify interactive elements Step 3 Apply natural language understanding to button labels Step 4 Reason "This green button labeled Submit Form is the submission control" Step 5 Execute click action on identified element Step 6 Scan for visual confirmation via success message or page transition
What happens when the EMR updates The button moves. The ID changes. The color scheme updates. Result Agent identifies the new button location using visual recognition. Workflow continues without interruption. No human intervention required.
The Unstructured Data Problem: Why RPA Fails at Intake
Let me show you a real scenario that breaks traditional automation every single time.
Let me show you a real scenario that breaks traditional automation every single time.
The Referral A hospital discharge planner faxes you a referral at 447 PM on a Friday. The patient is being discharged on Monday morning and needs admission that day. The referral includes a face sheet that is crooked and a handwritten physician's order and an insurance card photo with glare.
What RPA does Document 1 Face Sheet. Successfully extracts patient name and date of birth using OCR. Fails to extract the address because the scan cut off the bottom 20% of the page. Flags for manual review. Document 2 Physician Order. OCR returns gibberish because the handwriting is not machine-readable. "Home health 3x week" becomes "Hone halt 5v rock". Flags for manual review. Document 3 Insurance Card. OCR reads the member ID as "H32956B1" when it is actually "H82956B1" due to glare. The bot enters an incorrect ID into EMR. The claim will be denied in 45 days. Error undetected.
Final result 3 out of 4 documents flagged for manual review. One critical data error goes undetected. Your intake coordinator spends 35 minutes manually processing what was supposed to be automated.
What a GenAI Agent does Document 1 Face Sheet. Vision model detects that the document is cropped. The agent reasons that the address field is incomplete. The agent cross-references the patient name with publicly available address databases. Finds three potential matches. Flags ambiguity and suggests the most likely option based on hospital location proximity. Document 2 Physician Order. LLM reads handwritten text using advanced OCR and contextual reasoning. "Hone halt 5v rock" is evaluated against medical terminology. Agent infers "Home health 3x week" based on context and medical standards. Confidence score 94%. Auto processes. Document 3 Insurance Card. Vision model detects glare on a specific region of the image. The agent applies image preprocessing to reduce glare. Reads corrected member ID as "H82956B1". Cross validates against insurance company database format rules. Auto processes.
Final result 4 out of 4 documents processed automatically. Zero manual review required. The patient was admitted on Monday morning as scheduled.
The Maintenance Trap: How Much Are You Really Paying?
Most agencies do not track the true cost of RPA maintenance because it is hidden across multiple budget lines.
Let me show you the real math.
Scenario A 30-staff agency with 3 RPA bots Bot 1 Intake automation Bot 2 OASIS pre-fill Bot 3 Billing and claims submission
Annual maintenance cost $20,000 Downtime revenue loss $192,000 Staff overtime $15,200
Total cost of ownership $245,200 per year Original promised ROI Save $60,000 in staff costs Actual result Net loss of $185,200
This is the fragility trap.
Stop Paying for Maintenance. Start Paying for Results.
True automation means resilience.
It means software that can handle a messy and unstructured and constantly updating world without needing a developer to hold its hand every time a vendor pushes an update.
Copper Digital agents reduce admin costs by 60%.
Not because they are cheaper than RPA. Because they actually work when the EMR changes. Because they can read a crooked fax. Because they can reason through ambiguity instead of throwing an error and shutting down.
The difference is clear. RPA asks "Is this pixel exactly where I expect it to be?" GenAI asks "What is the user trying to accomplish and how do I help them do it?"
One is fragile. The other is resilient.
The Real Question
If you have to fix your automation every month is it really automation?
Or is it just a very expensive macro that breaks whenever the wind changes?
Your competitors are already making the switch. The national operators have spent millions building AI-powered operations platforms. They are processing referrals in 20 minutes while you are waiting 3 days for a vendor to patch a broken script.
They are winning the referrals. They are scaling faster. They are spending less on overhead. Referral leakage is costing you 10-30% of your potential revenue while you wait for bots to be fixed.
You can stay on RPA and keep paying for patches.
Or you can upgrade to autonomous agents that adapt instead of breaking.
The choice is yours.
But the discharge planners who are calling your competitors instead of waiting for your callback? They have already decided.
Frequently Asked Questions
What is the difference between RPA and AI Agents?
RPA is rule-based software that mimics clicks on a screen and breaks if the screen changes. AI Agents use computer vision and machine learning to understand the screen, allowing them to adapt to changes without crashing.
Why does home health need GenAI instead of RPA?
Home health deals with unstructured data like faxes, handwritten notes, and non-standardized forms. RPA cannot read these documents reliably. GenAI can extract data from them with near-human accuracy, regardless of format or quality.
Does Copper Digital use RPA?
No. Copper Digital uses autonomous AI Agents that integrate directly with EMRs and use cognitive processing to handle complex tasks like intake, coding, scheduling, and billing. Our agents do not break when your EMR updates.
How much does downtime really cost?
For a typical 30-staff agency, each day of automation downtime costs approximately $3,800 in lost productivity, overtime, and delayed referrals. Annual downtime from RPA failures averages $190,000 to $240,000.
Can AI agents work with any EMR?
Yes. Because they use computer vision and semantic understanding instead of code inspection, they can work with any web-based interface, including WellSky, Axxess, Homecare Homebase, KanTime, and custom systems.
Next Steps
Stop patching broken scripts. Upgrade to a workforce that thinks.
Schedule a 20-minute RPA Fragility Assessment.
We will review your current automation stack and show you how many maintenance incidents you are experiencing annually and calculate your true total cost of ownership including downtime.
Book Your Assessment
Copper Digital Autonomous AI Agents for Home Health Agencies That Refuse to Pay for Broken Scripts

