Blog
Jan 16, 2026
All-Payer OASIS Requirements 2026: What Home Health Agencies Need to Know

Arvind Sarin

If you run a Medicare-certified home health agency, your documentation workload just got significantly larger. And it is not going back.
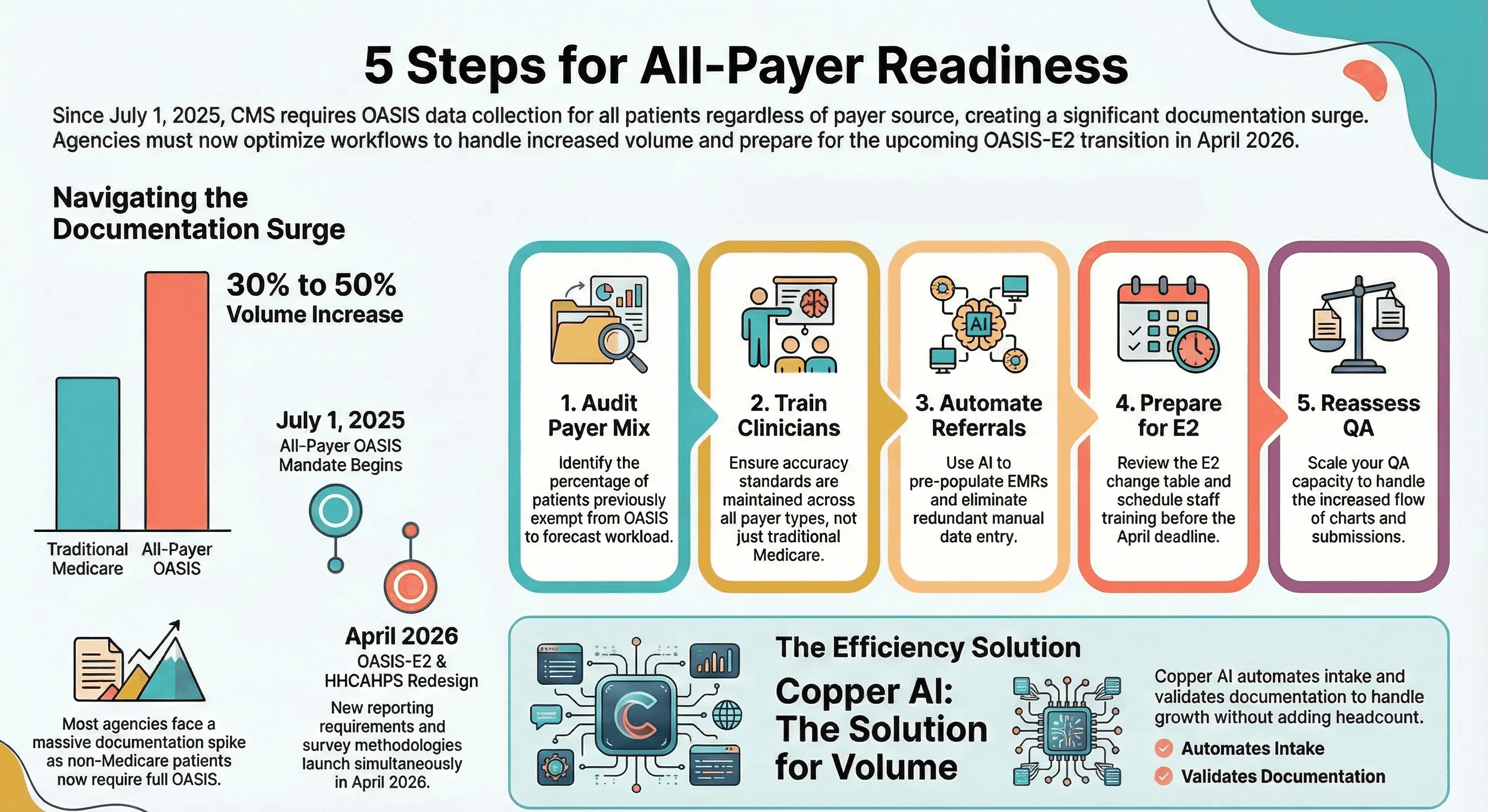
Since July 1, 2025, CMS has required OASIS data collection and submission for all patients regardless of payer source. Every Medicare Advantage patient. Every Medicaid patient. Every commercial insurance patient. Every self-pay patient. Even patients receiving care at no charge.
If your agency is providing skilled services to an adult for more than one visit, you must complete and submit OASIS to iQIES. No exceptions based on who is paying the bill.
This is not a minor policy tweak. It is a fundamental change in the volume of documentation your clinicians are responsible for. And with OASIS-E2 arriving in April 2026 and a redesigned HHCAHPS survey launching the same month, the documentation demands on home health agencies are about to compound.
Here is what the all-payer mandate actually means for your operations, and what you should be doing about it right now.
Why CMS Made This Change
For years, home health agencies only submitted OASIS assessments for Medicare and Medicaid patients. Everyone else, including Medicare Advantage, commercial payers, and self-pay, was excluded from OASIS reporting.
That created a blind spot. CMS could measure quality outcomes for traditional Medicare patients, but had no standardized data on the rest. Given that more than 54 percent of eligible Medicare beneficiaries are now enrolled in Medicare Advantage plans, that blind spot had become a crater.
The all-payer mandate closes it. CMS now has a unified data set to compare outcomes, measure quality, and build future payment models across all payer types. The agency has stated its intent to gain “a better understanding of the overall quality of care provided by Medicare-certified providers to the patients they serve, regardless of the patient’s payer source.”
This is not the end of the road. It is the foundation for what comes next. Expect all-payer OASIS data to eventually feed into quality measures, star ratings, and Value-Based Purchasing calculations. The agencies that treat this as a compliance checkbox today will be caught off guard when CMS ties it to reimbursement tomorrow.
The Timeline You Need to Know
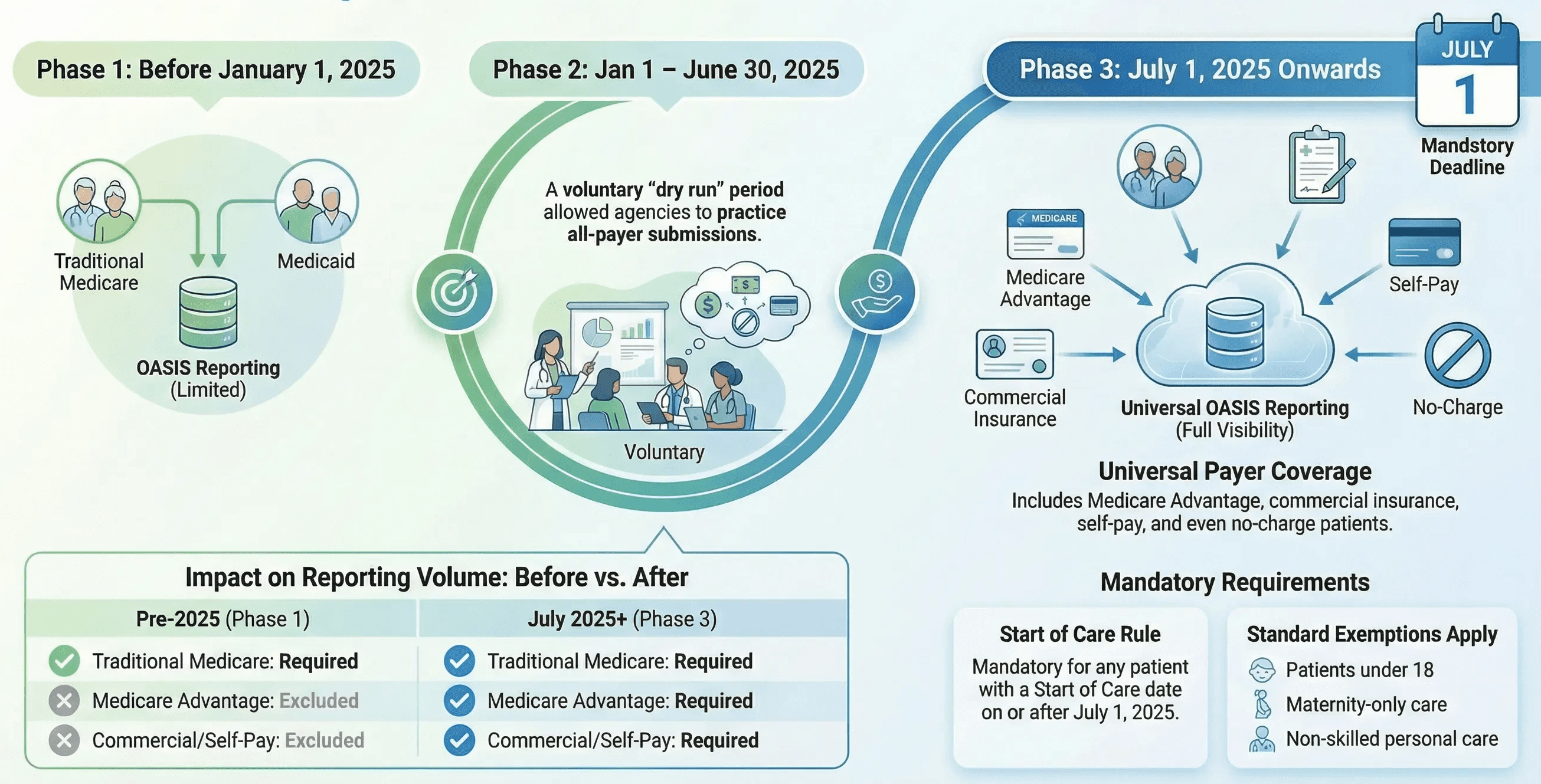
The rollout happened in three phases.
Before January 1, 2025: OASIS was required only for Medicare and Medicaid patients receiving skilled services. Non-Medicare and non-Medicaid patients were excluded from OASIS submission. Any OASIS submitted for these patients would be rejected by iQIES.
January 1 through June 30, 2025: CMS opened a voluntary phase-in period. Agencies could begin collecting and submitting OASIS for non-Medicare and non-Medicaid patients, but it was optional. This was a dry run. OASIS data collected during this voluntary period does not count toward quality measures or HHVBP Model calculations.
July 1, 2025, onward: Mandatory. For any patient with a Start of Care date on or after July 1, 2025, OASIS data collection and submission are required for all payer sources. This includes all subsequent assessments: resumption of care, recertification, transfer, discharge, and death at home.
One important nuance: patients who began care before January 1, 2025, under a non-Medicare and non-Medicaid payer do not require OASIS retroactively. The mandate applies based on the Start of Care date, not the current date.
Who Is Exempt
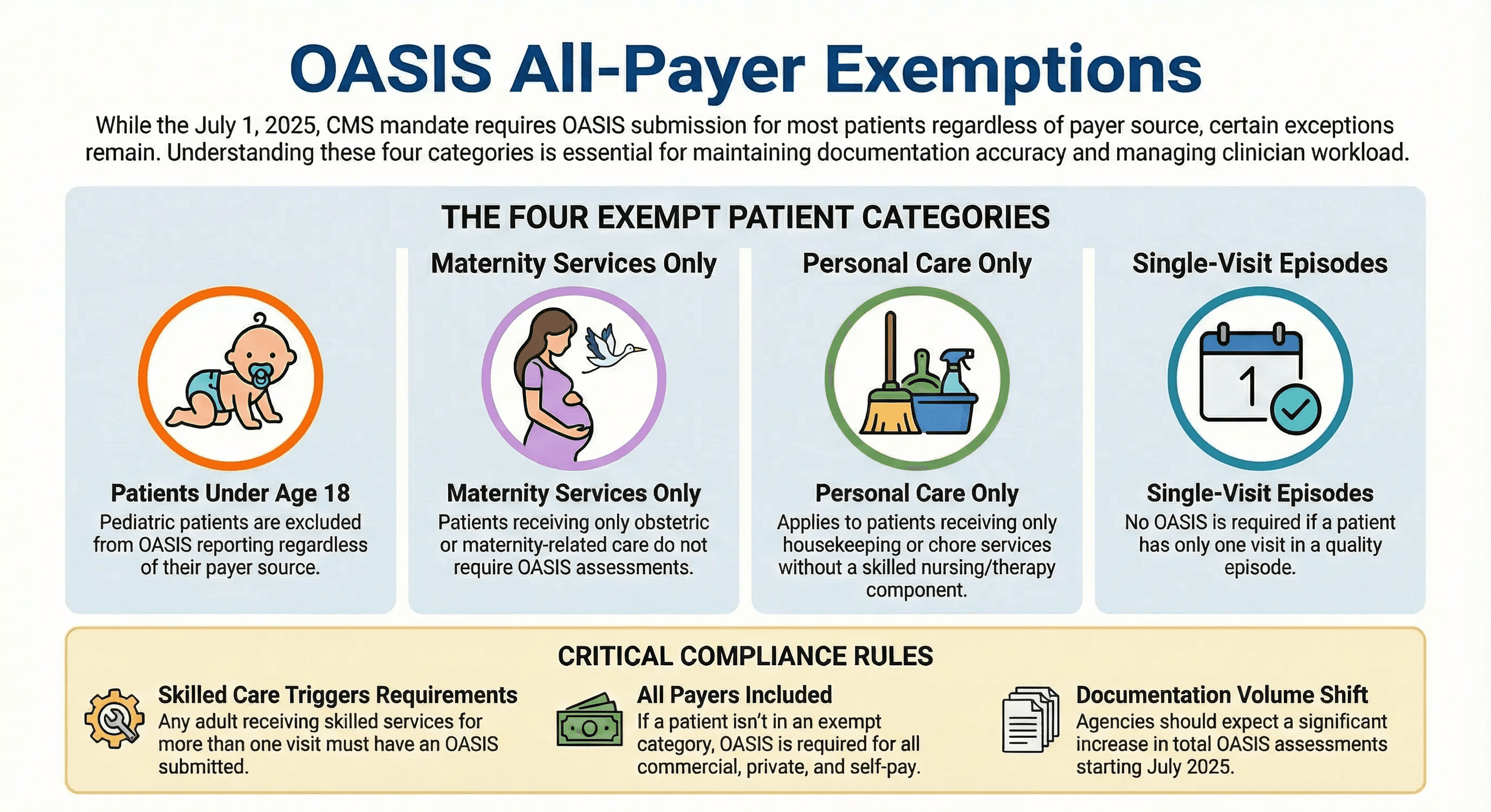
The exemptions have not changed. Three categories of patients remain excluded from OASIS regardless of payer:
Patients under 18 years of age. Patients receiving only maternity services. Patients receiving only personal care, housekeeping, or chore services without any skilled nursing or therapy component.
There is also the single-visit exception. If a patient has only one visit in a quality episode, such as a single evaluation where the patient refuses further care, no OASIS is required, and no discharge OASIS should be completed.
Everyone else who is receiving skilled services from a Medicare-certified agency needs a full OASIS. No matter who pays.
The Operational Impact Most Agencies Underestimate
The policy is simple. The operational impact is not.
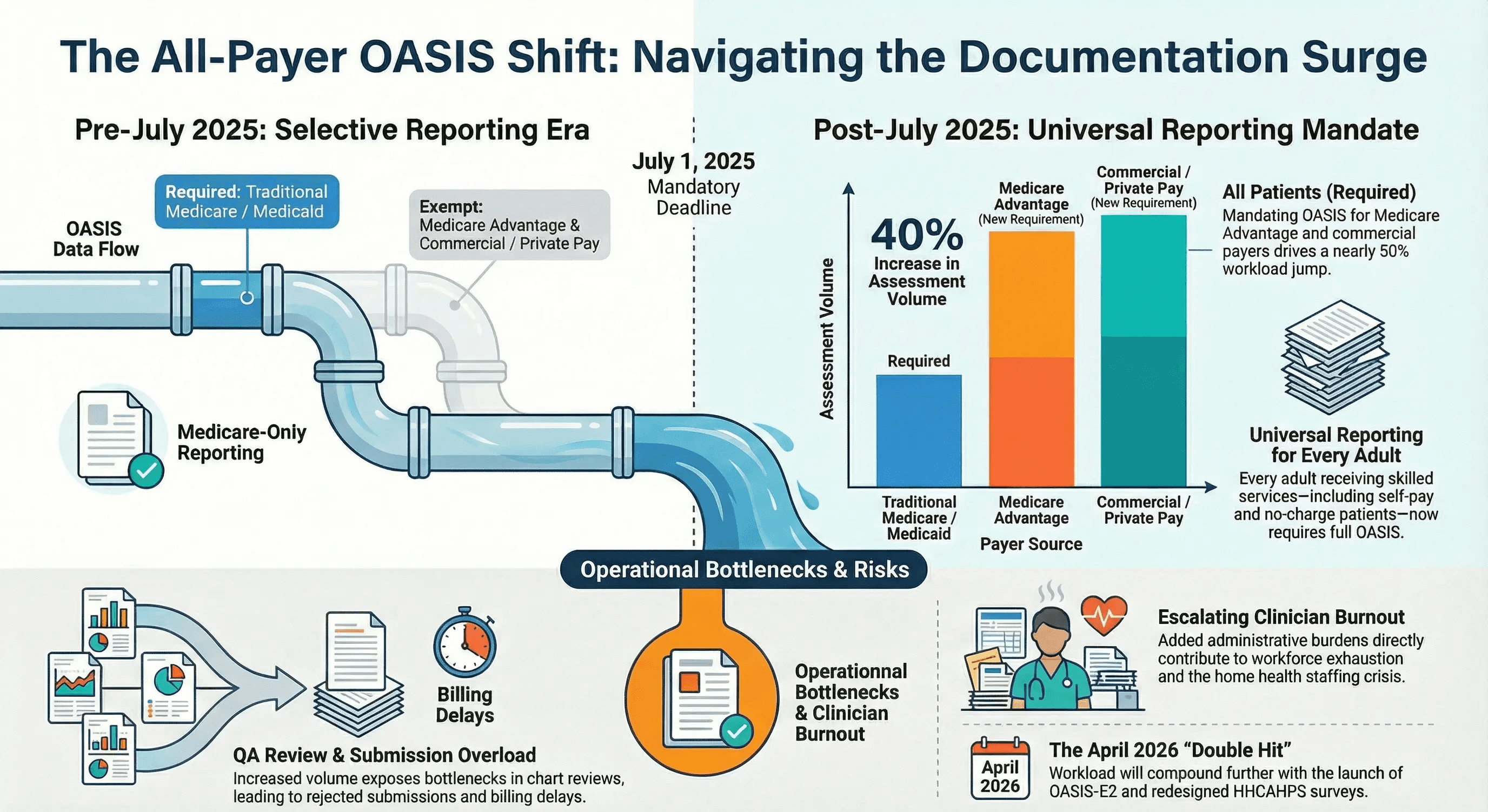
Most home health agencies were already stretched thin on documentation capacity. The all-payer mandate does not add new complexity to each OASIS assessment. What it adds is volume.
Consider an agency where 40 percent of patients are covered by Medicare Advantage, commercial insurance, or self-pay. Before July 2025, those patients did not require OASIS. Now they do.
That is a 40 percent increase in the number of OASIS assessments your clinicians must complete. Same staff. Same hours. Significantly more documentation.
Here is where that volume shows up:
Start of Care assessments. Every new admission now triggers a full OASIS, regardless of payer. If your agency admits 50 patients per week and 20 of them were previously non-OASIS payers, your clinicians are now completing 20 additional comprehensive assessments every week.
Subsequent time points. The mandate does not stop at the start of Care. Recertifications, resumptions of care, transfers, and discharges all require OASIS for all-payer patients. This compounds over time as patients move through their episodes.
QA and submission volume. More OASIS assessments mean more charts flowing through your QA team, more submissions to iQIES, and more potential for rejection or error. If your QA process is already a bottleneck, the all-payer mandate will expose it.
Clinician time. The U.S. Surgeon General’s advisory on health worker burnout identified administrative burden as a leading driver of workforce exhaustion. Adding OASIS to every patient adds directly to that burden.
What Changes with OASIS-E2 in April 2026
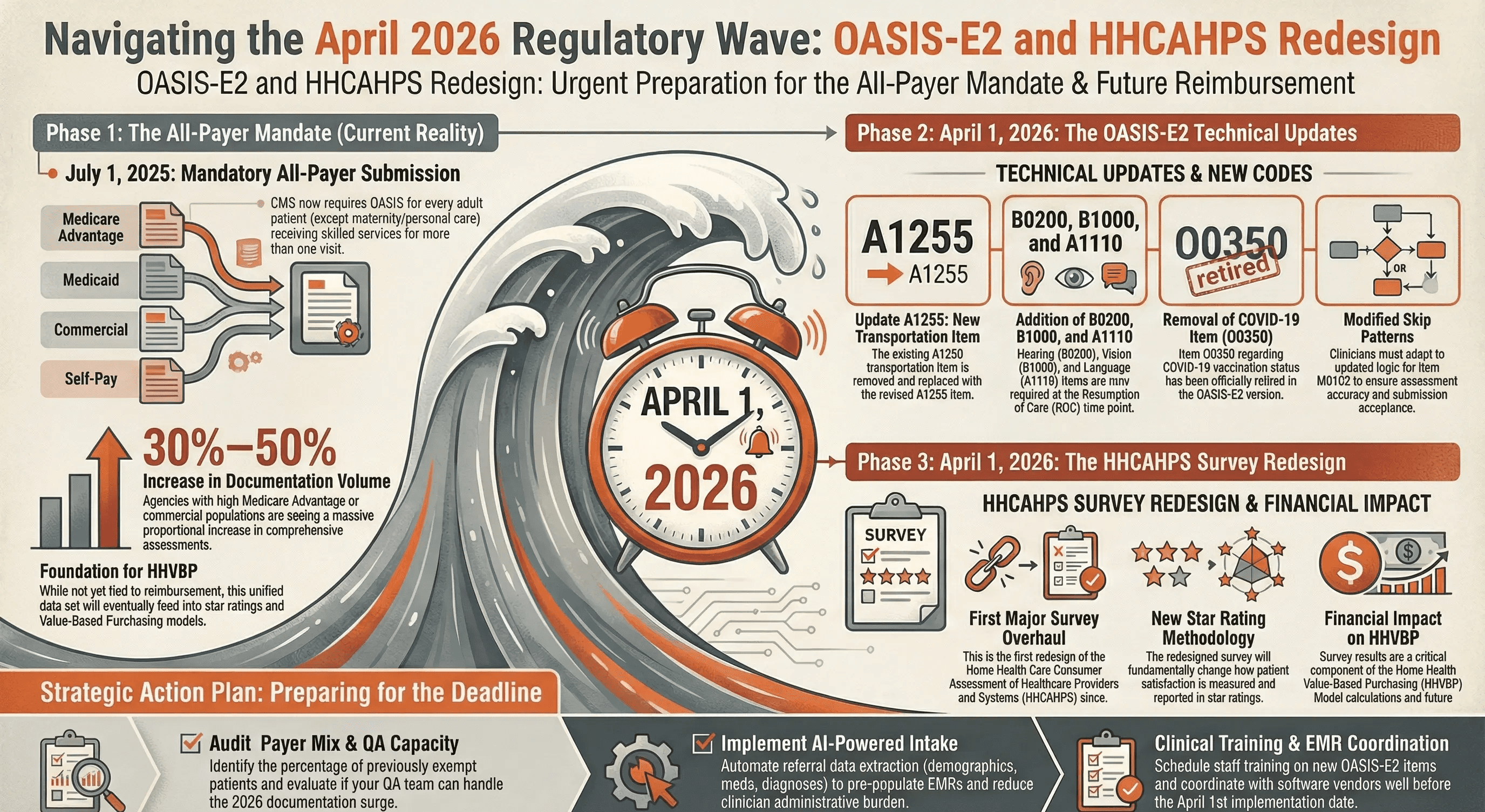
On top of the all-payer volume increase, CMS is rolling out OASIS-E2 effective April 1, 2026. This is a refinement rather than an overhaul, but it still requires attention.
The key changes include the removal of the COVID-19 vaccination item (O0350), a revised transportation item replacing A1250 with a new A1255, the addition of hearing (B0200), vision (B1000), and language (A1110) items to the resumption of care time point, and a modified skip pattern for M0102.
Separately, the HHCAHPS survey is being redesigned for the first time since its original implementation, also launching in April 2026. The new survey will change the star rating methodology and will have a significant impact on HHVBP Model calculations.
Agencies are facing a double hit in April 2026. New OASIS items and workflows coinciding with a new patient satisfaction measurement system. Both will affect reimbursement. Both require preparation now.
5 Things to Do Right Now
1. Audit Your Current Payer Mix
Pull a report on your patient population by payer type. Identify what percentage of your patients were previously exempt from OASIS and are now subject to the mandate. This gives you a clear picture of how much additional documentation volume you are absorbing.
If Medicare Advantage and commercial patients represent 30 to 50 percent of your census, you are looking at a proportional increase in OASIS workload that your current staffing model was not designed to handle.
2. Train Clinicians on All-Payer Expectations
Your field staff needs to understand that OASIS quality standards apply equally across all payers. The temptation is to treat non-Medicare OASIS assessments as lower-priority paperwork. That would be a mistake.
CMS has not yet announced specific quality measures tied to all-payer data. But the infrastructure is being built. All-payer OASIS data will eventually flow into outcome calculations. Agencies that establish accuracy standards now will be ahead when CMS flips that switch.
3. Automate Referral Data Extraction
The single most effective way to absorb a volume increase without adding headcount is to eliminate redundant data entry.
AI-powered intake automation can read referral documents, discharge summaries, and physician orders and pre-populate the EMR with patient demographics, diagnosis codes, medication lists, and insurance information. When the clinician opens the chart, the work has already started.
This is not a nice-to-have. When you are doing OASIS on every patient, the time savings from automated data extraction scale proportionally with the mandate.
4. Prepare for OASIS-E2 Now
Do not wait until April. Review the OASIS-E2 change table and identify which items affect your workflows. Coordinate with your EMR vendor on software updates. Schedule clinician training before the April 1 implementation date.
The agencies that scramble to learn new items while simultaneously absorbing all-payer volume will make errors. Errors lead to rejected submissions, rework, and delayed billing.
5. Reassess Your QA Capacity
If your QA team was sized for Medicare-only OASIS volume, it is undersized for all-payer volume. Evaluate whether your current QA workflow can handle the additional chart reviews. Consider AI-powered validation tools that can flag inconsistencies between OASIS scores and clinical narratives before submission, reducing the return-and-fix cycle.
The Bigger Picture
The all-payer OASIS mandate is not an isolated regulation. It is part of a deliberate CMS strategy to build a unified quality measurement system across all of home health.
Combined with the HHVBP expansion, the HHCAHPS redesign, and the ongoing shift toward value-based reimbursement, the message from CMS is clear. Documentation accuracy and efficiency are no longer just operational concerns. They are financial ones.
The agencies that scale their documentation capacity through automation will absorb these changes without breaking their workforce. The agencies that try to handle it manually will burn out their best clinicians and fall behind.
Copper Digital builds AI agents that automate the intake and documentation workflow for home health agencies. We help you absorb volume increases without adding headcount by eliminating redundant data entry and validating documentation before submission.
See how Copper AI helps agencies handle the all-payer mandate →

