Blog
Apr 23, 2026
The Denial Management Playbook for Home Health Agencies

Arvind Sarin, CEO& Chairman of Copper Digital

We talk to agency owners every week who describe the same pattern. The billing team is overwhelmed. There is a growing pile of denied claims that nobody has time to appeal. The ones that do get appealed are submitted late because the documentation has to be pulled from multiple systems. And by the time anyone analyzes why the denials happened, three more months of the same errors have already been billed and denied. The agency is hemorrhaging recoverable revenue while the clinical team keeps charting the same way that caused the problem.
Denial management is not a billing function. It is an operational discipline that starts at intake, runs through every clinical visit, and ends with a clean claim that never gets denied in the first place. The agencies that have their denial rates under control are not better at writing appeals. They are better at preventing the need for appeals.
Where Home Health Denials Actually Come From
The top denial triggers in home health have not changed meaningfully in years, which tells you something about how deeply embedded they are in the operational workflow.
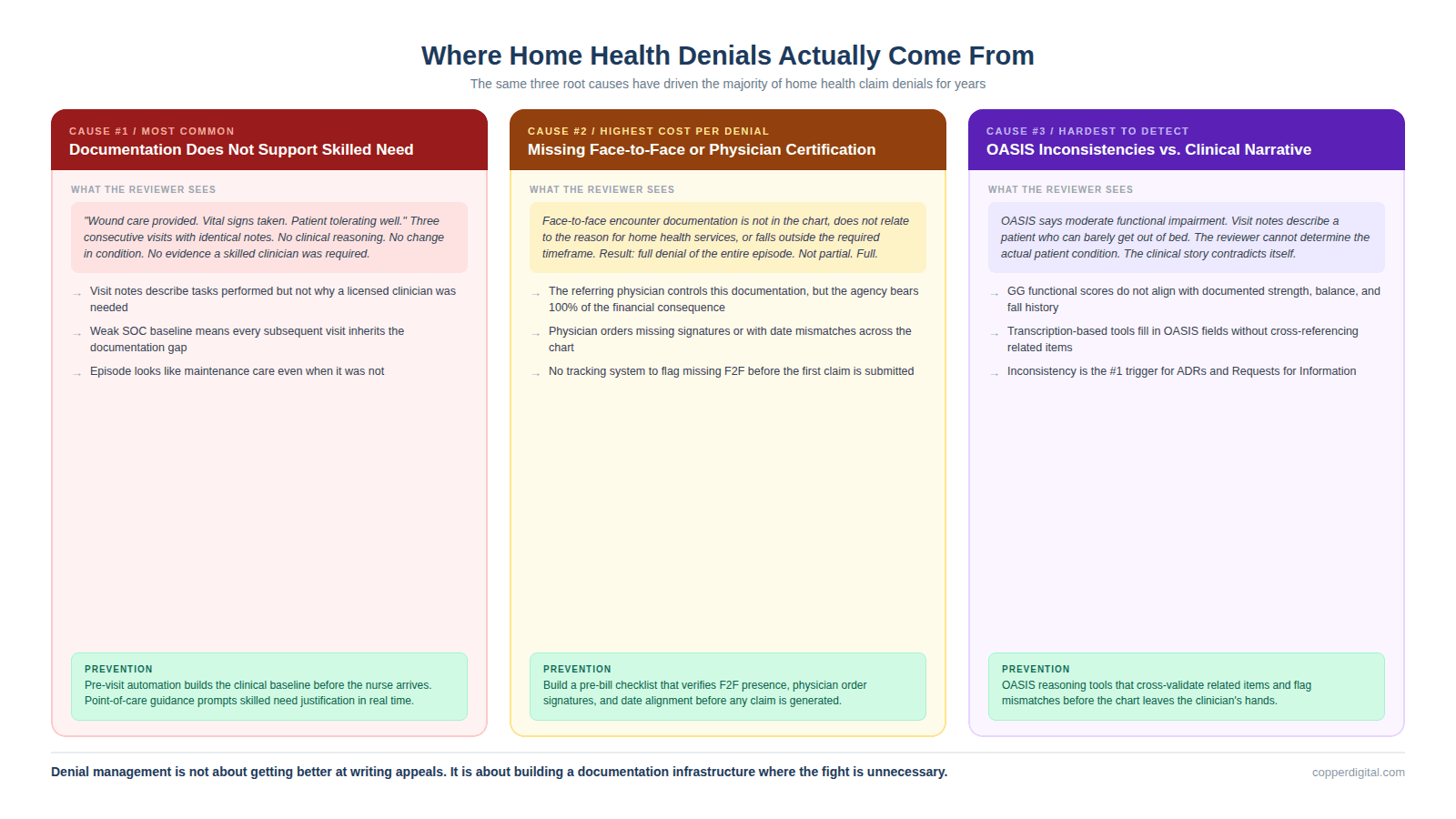
Documentation Does Not Support Medical Necessity or Skilled Need
This is the number one reason home health claims are denied, and it is the one most agencies struggle with the longest. The clinical note describes what the nurse did during the visit, but it does not clearly establish why that visit was medically necessary or why it required the skills of a licensed clinician rather than a home health aide. A reviewer reads three consecutive visit notes that say wound care provided, vital signs taken, patient tolerating well, and sees no clinical reasoning, no change in condition, and no evidence that a skilled clinician was required. The care was probably excellent. The documentation made it invisible.
This problem compounds across episodes. If the start of care assessment does not clearly document the patient's baseline functional limitations, the clinical justification for skilled services is weak from the beginning. Every subsequent visit note inherits that weakness. And when the claim is selected for an Additional Documentation Request, the reviewer sees an episode that looks like maintenance care rather than skilled care, even when it was not.
Missing or Incomplete Physician Certification and Face-to-Face Encounter
The physician must certify that the patient needs skilled nursing, therapy, or both, that the patient is homebound, and that a plan of care has been established. The face-to-face encounter must occur within specified timeframes and must relate to the primary reason the patient needs home health services. When the face-to-face documentation is missing, incomplete, or does not connect to the reason for home health services, the claim is denied outright. This is not a partial denial. It is a full denial of the entire episode.
Agencies get caught here because the face-to-face encounter is completed by the referring physician, not by the agency's clinicians. The agency has limited control over the quality and timeliness of that documentation. But the agency bears 100% of the financial consequence when it is missing. Building a workflow that tracks face-to-face documentation status before the first claim is submitted is the most straightforward prevention step, and most agencies still do not have one.
OASIS Inconsistencies That Contradict the Clinical Narrative
When the OASIS assessment says the patient is moderately impaired on functional items but the visit notes describe someone who can barely get out of bed, the reviewer sees a mismatch. That inconsistency triggers a denial because the documentation does not tell a coherent clinical story. Either the OASIS is wrong, the visit notes are wrong, or the clinician did not connect the two. In any case, the reviewer cannot determine what the actual patient condition was, and the claim is denied.
This is where the distinction between OASIS transcription and OASIS reasoning matters operationally. A tool that simply records what the clinician says and fills in OASIS fields does not catch when the GG0170 mobility score contradicts the documented lower extremity strength and fall history. A reasoning-based tool cross-references those items and flags the inconsistency before the chart leaves the clinician's hands.
How the ADR and TPE Process Actually Works
When your agency is selected for review, it starts with an Additional Documentation Request. An ADR is a formal request from a Medicare Administrative Contractor, CERT contractor, UPIC, or other review entity for the medical records supporting a specific claim. You have a defined window to respond, typically 45 days, and you must submit the records in the correct format and order. Leaving out a critical document or submitting records that are disorganized can result in a denial even when the underlying documentation is adequate.
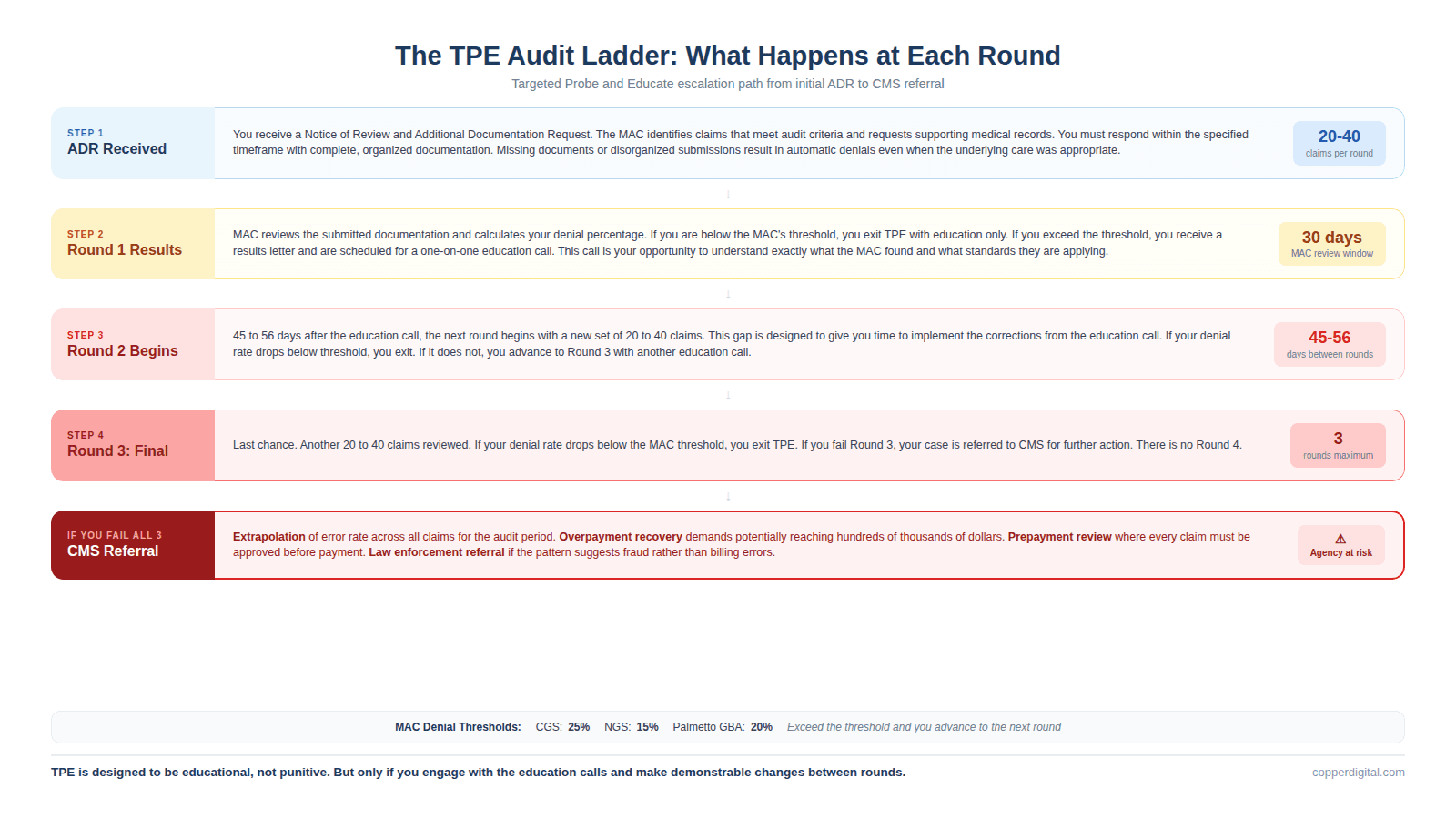
Targeted Probe and Educate is CMS's structured audit program designed to reduce improper payments through education rather than punishment. When your agency is selected for TPE, you receive a Notice of Review and will have 20 to 40 claims reviewed per round. At the end of each round, you receive a calculated denial percentage. Each MAC has a threshold: CGS requires you to be under 25%, NGS under 15%, and Palmetto GBA under 20%. If your denial rate exceeds the threshold, you advance to the next round. After a failed round, the MAC schedules an education call, and the next round begins 45 to 56 days later. If you fail all three rounds, you are referred to CMS for further action, which can include extrapolation and overpayment demands, prepayment review, or referral to law enforcement.
The critical thing to understand about TPE is that it is designed to be educational, not punitive, but only if you engage with it that way. The education call after a failed round is an opportunity to understand exactly what the MAC found, what documentation standards they are applying, and what specific changes they expect. Agencies that treat the education call as a checkbox rather than a genuine learning opportunity tend to fail subsequent rounds with the same errors.
The Five-Level Medicare Appeal Process
When a claim is denied, you have five levels of appeal available. Most agencies only use the first two, and many do not even use those consistently.
Level 1: Redetermination by the MAC. You have 120 days from the date of the initial determination to file. The MAC reviews the documentation again, often by a different reviewer. This is your first and fastest opportunity to reverse the denial, and it succeeds more often than agencies expect when you submit a clear, organized response with additional clinical context that addresses the specific denial reason.
Level 2: Reconsideration by a Qualified Independent Contractor (QIC). If the redetermination is unfavorable, you have 180 days to request reconsideration. The QIC is independent of the MAC and conducts a fresh review. This is where a well-constructed appeal with clinical rationale and supporting documentation can overturn a denial that survived Level 1.
Level 3: Hearing before an Administrative Law Judge (ALJ) at the Office of Medicare Hearings and Appeals. The claim must meet a minimum dollar threshold, which is $200 for 2026. You have 60 days after the QIC decision to request a hearing. ALJ hearings allow you to present testimony and are conducted by phone, video, or in person.
Level 4: Review by the Medicare Appeals Council. The minimum dollar threshold for 2026 is $1,960. You have 60 days after the ALJ decision to request review.
Level 5: Judicial review in federal district court. The minimum dollar threshold for 2026 is $1,960. This is the final level and is rarely used for individual home health claims, but it is available.
The reality is that most home health denials should be resolved at Level 1 or Level 2 if the documentation is adequate and the appeal is constructed properly. Agencies that allow denials to accumulate without filing timely appeals are voluntarily writing off revenue that could have been recovered.
Building a Pre-Bill Review Process That Prevents Denials
The most effective denial management strategy is not a better appeals workflow. It is a pre-bill review process that catches the errors before the claim is submitted.
What Pre-Bill Review Should Check
Physician orders: Are they signed, dated, and do the dates match across the chart? Are the verbal orders documented with the date received and sent for signature?
Face-to-face encounter: Is it present, does it relate to the primary reason for home health, and does it fall within the required timeframe?
OASIS consistency: Do the functional scores align with what the visit notes describe? Does the clinical narrative support the functional impairment level that drives PDGM payment?
Skilled need: Do the visit notes clearly establish why each visit required a licensed clinician rather than a home health aide? Is there clinical reasoning documented, not just tasks performed?
Homebound status: Is there a clear statement of why the patient meets the homebound criteria, and is it documented at the required frequency?
Plan of care: Is it individualized? Does it match the actual services being provided? Are wound care supplies and equipment listed accurately?
How Pre-Visit Automation Prevents Denials at the Source
Many of the documentation failures that cause denials originate before the nurse ever walks into the patient's home. The referral data was entered incorrectly at intake. The medication list was incomplete. The prior episode history was not reviewed. The physician's face-to-face encounter documentation was not tracked. These are pre-visit failures that contaminate every downstream document in the episode.
Copper Digital's pre-visit AI agents address this by extracting referral data using computer vision, verifying eligibility before the SOC visit, pre-populating the EMR with demographics, diagnoses, and medications, and flagging when face-to-face encounter documentation is missing before the first claim is generated. The intake that used to take 45 minutes of manual data entry, with all the transcription errors that come with it, now takes approximately 3 minutes with a clean data foundation. When the starting data is right, the downstream documentation has fewer inconsistencies, the OASIS aligns with the clinical picture, and the claim is defensible from the first submission.
Denial management is not about getting better at fighting payers. It is about building a documentation and billing infrastructure where the fight is unnecessary because the claim was clean from the start.
TL;DR
Most home health agencies treat denials as a billing department problem. They are not. Denials are the final symptom of documentation, coding, and workflow failures that started weeks or months earlier. The top three denial triggers in home health, which have remained consistent for years, are documentation that does not support medical necessity or skilled need, missing or incomplete physician certification and face-to-face encounter documentation, and OASIS inconsistencies that contradict the clinical narrative. This blog walks through where denials actually originate, how the ADR and TPE audit process works, the five-level Medicare appeal system, how to build a pre-bill review process that prevents denials before they happen, and how pre-visit automation addresses the root causes rather than the symptoms.
Frequently Asked Questions
What are the top reasons home health claims are denied?
The top three denial triggers in home health are documentation that does not clearly support medical necessity or skilled need, missing or incomplete physician certification and face-to-face encounter documentation, and OASIS scoring inconsistencies that contradict the clinical narrative. These three categories account for the majority of Traditional Medicare denials and have remained consistent over multiple years of TPE audit data.
What is a TPE audit in home health?
Targeted Probe and Educate is CMS's structured medical review program conducted by Medicare Administrative Contractors. When an agency is selected, the MAC reviews 20 to 40 claims per round. Each round produces a denial percentage that is compared against the MAC's threshold (CGS 25%, NGS 15%, Palmetto GBA 20%). Agencies exceeding the threshold advance to subsequent rounds with education calls in between. Failing all three rounds results in referral to CMS for further action including potential extrapolation, prepayment review, or law enforcement referral.
What is an ADR in home health?
An Additional Documentation Request is a formal request from a Medicare contractor for the medical records supporting a specific claim. ADRs can come from the MAC, CERT contractors, UPICs, or Supplemental Medical Review Contractors. The agency must respond within the specified timeframe, typically 45 days, with complete and organized documentation. Failure to respond or submitting incomplete records results in automatic denial of the claim.
How does the Medicare appeal process work for home health?
Medicare offers five levels of appeal. Level 1 is redetermination by the MAC (120 days to file). Level 2 is reconsideration by a Qualified Independent Contractor (180 days). Level 3 is a hearing before an Administrative Law Judge with a $200 minimum threshold for 2026. Level 4 is review by the Medicare Appeals Council with a $1,960 minimum threshold. Level 5 is judicial review in federal district court. Most home health denials should be resolved at Level 1 or Level 2 when documentation is adequate and the appeal addresses the specific denial reason.
How can agencies prevent denials before they happen?
The most effective denial prevention strategy is a pre-bill review process that checks physician orders, face-to-face encounter documentation, OASIS consistency, skilled need justification, homebound status, and plan of care accuracy before the claim is submitted. Pre-visit automation from Copper Digital addresses root causes by extracting referral data accurately, pre-populating the EMR with verified information, and flagging missing documentation before the first claim is generated. When the starting data is clean, downstream documentation has fewer inconsistencies and claims are defensible from the first submission.
What happens if you fail all three TPE rounds?
If an agency fails all three rounds of Targeted Probe and Educate, the MAC refers the case to CMS for further action. CMS may impose extrapolation of the error rate across all claims for the audit period, demand overpayment recovery, place the agency on prepayment review where every claim must be reviewed before payment, or refer the case to law enforcement if the pattern suggests fraud rather than billing errors. This is why engaging seriously with the education calls between rounds and making demonstrable operational changes is critical.
If your denial rate is climbing or you are preparing for a TPE round, request a free intake-to-billing assessment at copperdigital.com/contact-us. We will trace your denial patterns back to their root causes and show you where pre-visit automation can prevent them.

