Blog
Jan 23, 2026
Home Health Start of Care Documentation: A Complete Guide

Arvind Sarin

The Start of Care visit is the most important and most time-consuming event in a home health episode. It sets the clinical baseline, determines your reimbursement, establishes the care plan, and shapes every subsequent assessment for that patient.
It is also where most agencies lose the most time, make the most errors, and burn out their best clinicians.
This guide covers everything involved in a home health Start of Care: what is required, what takes the most time, what goes wrong, and how to fix it.
What Is a Start of Care in Home Health
The Start of Care is the initial comprehensive assessment conducted when a patient is admitted to home health services. Under 42 CFR §484.55, every Medicare-certified home health agency must provide a patient-specific comprehensive assessment that includes the OASIS data set.
The Start of Care visit is not just a clinical encounter. It is a regulatory event. The data collected during this visit determines your Patient-Driven Groupings Model (PDGM) classification, which directly controls how much Medicare pays for the episode. It feeds into your quality measures on Medicare Care Compare. And it establishes the clinical narrative that must hold up under audit.
For clinicians, the Start of Care is typically the longest visit they will perform. For agencies, it is the visit most likely to generate QA rework, billing delays, and compliance risk.
Who Can Complete a Start of Care Assessment
Not every clinician is qualified to complete a Start of Care OASIS.
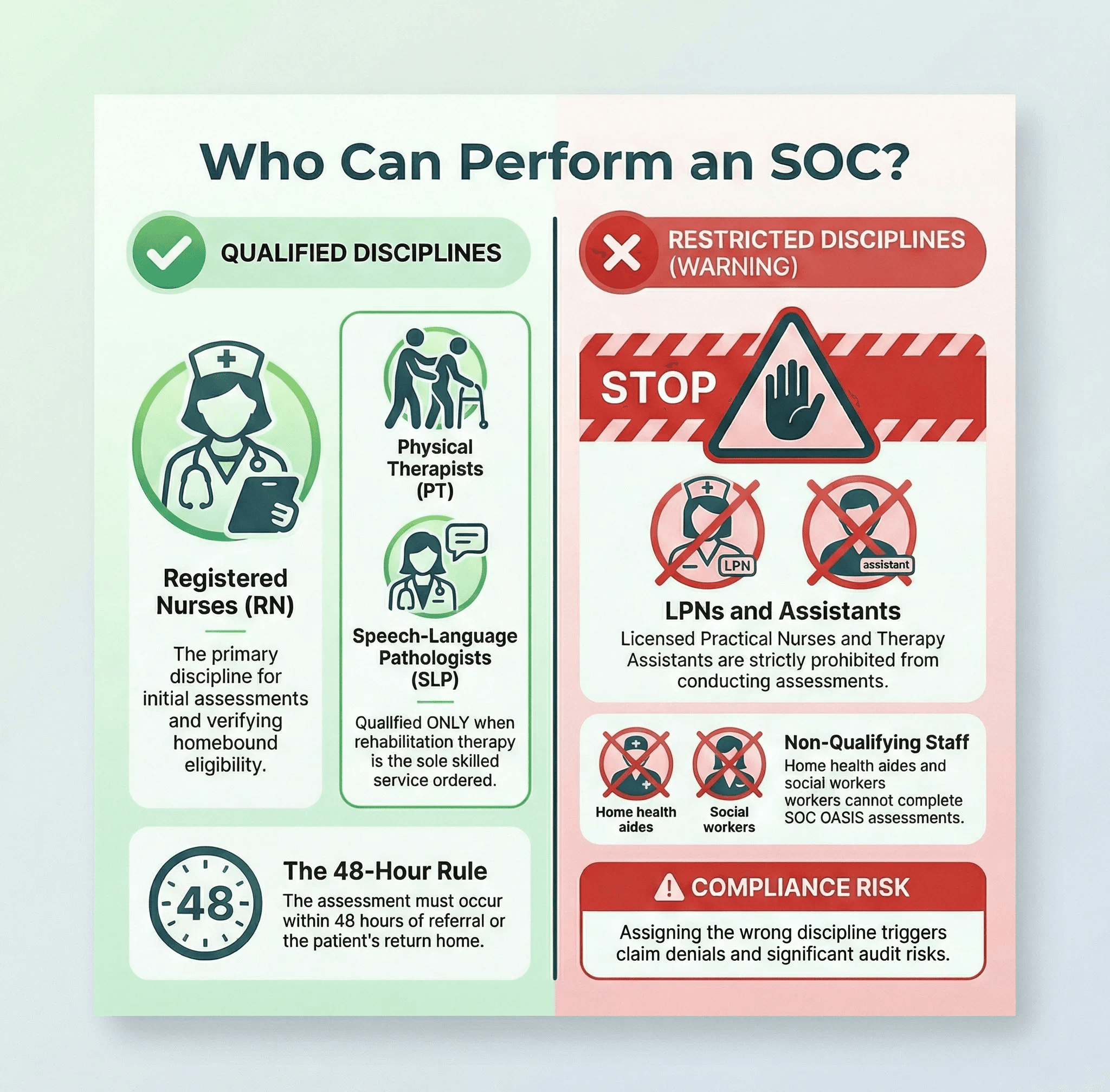
Under CMS regulations, a registered nurse must conduct the initial assessment visit to determine the patient’s immediate care needs and, for Medicare patients, to verify eligibility for the home health benefit, including homebound status. This initial assessment must occur within 48 hours of referral, within 48 hours of the patient’s return home, or on the physician-ordered start of care date.
When rehabilitation therapy is the only skilled service ordered, a physical therapist or speech-language pathologist may perform the initial assessment. Occupational therapists can participate in assessments, but Medicare does not recognize occupational therapy alone as a qualifying service for initiating home health.
Licensed practical nurses, home health aides, therapy assistants, and social workers cannot complete OASIS assessments. Assigning the wrong discipline creates compliance risk and can trigger claim denials.
What the Start of Care Assessment Must Include
The comprehensive assessment at Start of Care must cover a broad range of clinical and functional domains. Under the Conditions of Participation, the assessment must identify or evaluate:
The patient’s current health status, including clinical condition, comorbidities, and medication regimen. Psychosocial, functional, and cognitive status. The patient’s strengths, goals, and care preferences. Measurable outcome goals identified by the home health agency. Activities of daily living and instrumental activities of daily living. The patient’s primary caregiver, their willingness and ability to provide care, and their availability. The patient’s living situation, including safety hazards and supportive assistance available. Sensory status, integumentary status, respiratory status, elimination status, and neuro-emotional-behavioral status.
In practice, the Start of Care OASIS assessment contains over 100 data items spanning demographics, patient history, clinical status, functional scoring (Section GG), medication management, wound assessment, cognitive screening (BIMS), depression screening (PHQ-2/PHQ-9), social determinants of health, and discharge planning.
Each item must be scored accurately because the data drives PDGM payment classification, quality measure calculations, and public reporting on Medicare Care Compare.
The OASIS Time Points After Start of Care
The Start of Care is the first in a series of required OASIS assessment points throughout a patient’s home health episode. Understanding the full sequence matters because documentation decisions made at Start of Care cascade through every subsequent assessment.
Start of Care (SOC). The initial comprehensive assessment establishes the baseline. Must be completed within five days of the first home visit.
Resumption of Care (ROC). Required within 48 hours of a patient’s return home from an inpatient facility stay of 24 hours or more. This is essentially a second Start of Care and carries a similar documentation burden.
Recertification. Required in the last five days of every 60-day episode when continued home health care is needed. Reassess the patient’s status against the baseline established at Start of Care.
Transfer. Completed when a patient is transferred to an inpatient facility.
Discharge. Completed when the patient is discharged from home health services or when a patient dies at home.
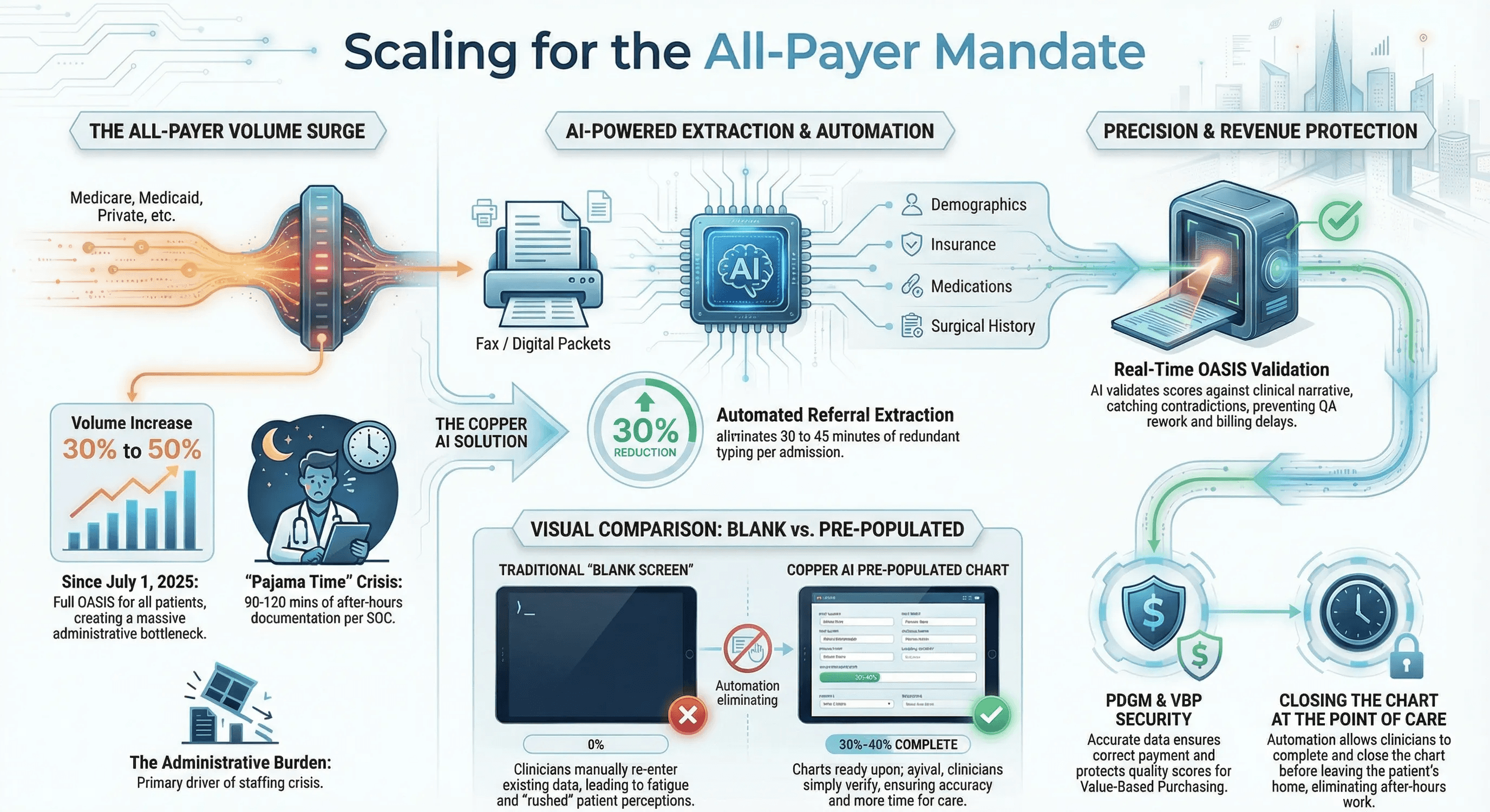
Since July 2025, all of these time points require OASIS completion for all patients, regardless of payer source, not just Medicare and Medicaid. This all-payer mandate has significantly increased the total volume of OASIS assessments agencies must complete.
Why Start of Care Documentation Takes So Long
If you ask your scheduling coordinator, a Start of Care visit takes two hours. If you ask the nurse who performed it, the honest answer is closer to six.
The scheduled visit time only accounts for the in-home portion. It does not account for the hours of work that happen before and after.
Pre-visit preparation (30 minutes). Before the nurse arrives at the patient’s home, she needs to review the referral packet, extract demographic and clinical information from faxed hospital discharge summaries, confirm the patient's address, verify insurance information, and map the route. Most of this time is spent manually reading and re-entering data that already exists in a document.
In-home clinical care (30 minutes). This is the actual nursing work: physical assessment, heart and lung sounds, wound evaluation, medication review, patient education, and safety assessment. This is the part of the visit that generates value for the patient.
In-home documentation (60 minutes). After the hands-on care, the nurse shifts to the tablet or laptop. She clicks through OASIS fields, enters diagnosis codes, scores functional items, and begins the clinical narrative. The patient sits waiting. Patients often report in HHCAHPS surveys that their nurse seemed distracted or rushed, even when the visit lasted two full hours.
After-hours charting (90 to 120 minutes). The nurse leaves the home with a chart that is 50 to 60 percent complete. After dinner, she opens her laptop and finishes the OASIS. The American Medical Association calls this after-hours documentation burden “pajama time.” It is one of the primary drivers of clinician dissatisfaction and burnout.
The total: roughly five to six hours of clinician labor for a visit that was scheduled for two. The U.S. Surgeon General’s advisory on health worker burnout identifies administrative burden as a leading contributor to the health worker staffing crisis. Start of Care documentation is one of the clearest examples.
The 5 Most Common Start of Care Documentation Errors
Documentation errors at Start of Care do not just affect the initial assessment. They cascade through the entire episode, affecting recertification accuracy, discharge outcomes, quality scores, and payment.
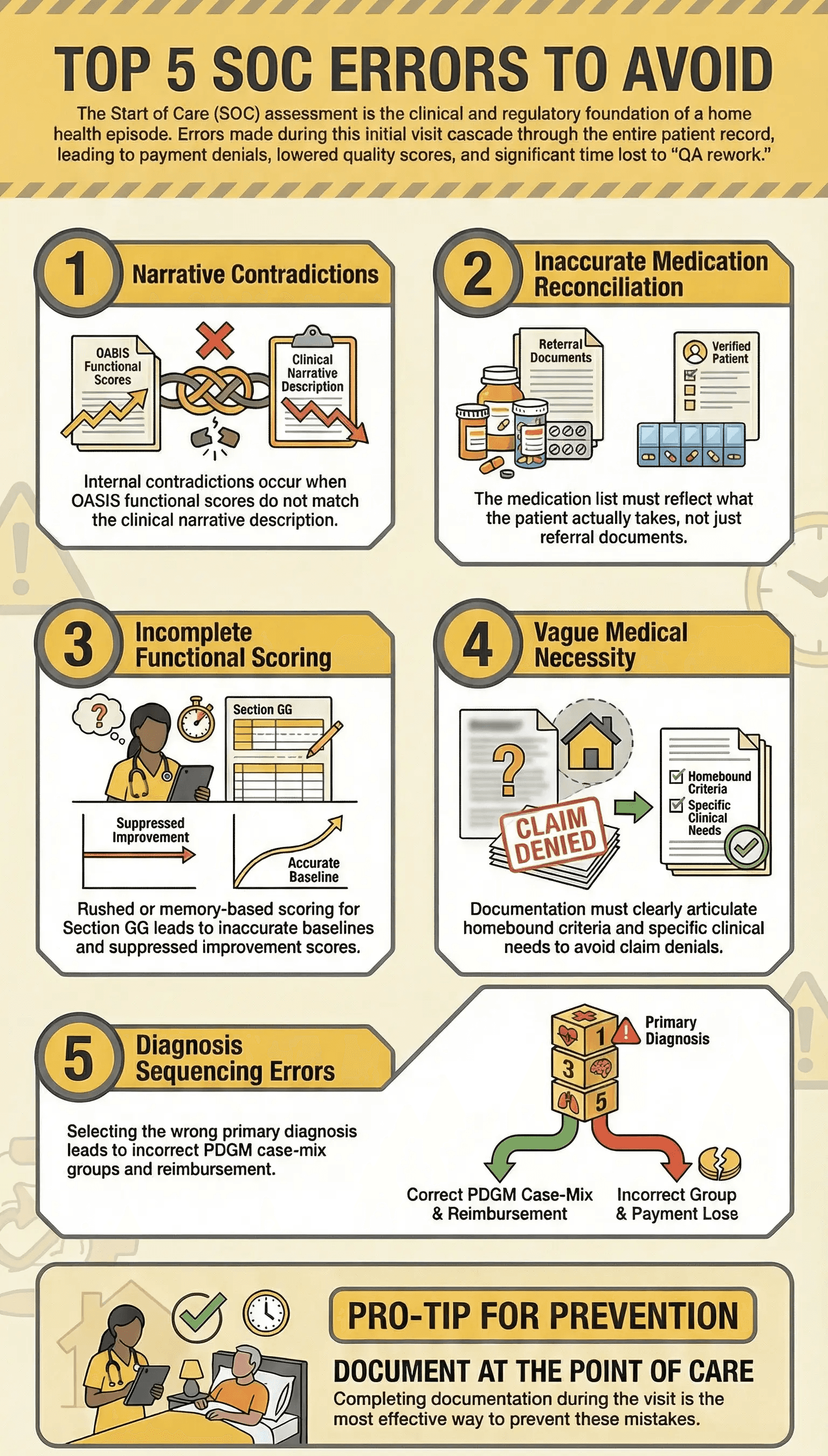
1. OASIS scores that do not match the clinical narrative. If the functional score says a patient requires moderate assistance with bathing, but the narrative describes the patient as independent, the chart has an internal contradiction. This is the number one trigger for QA returns and the most common reason charts are sent back for correction.
2. Inaccurate medication reconciliation. The medication list at Start of Care must reflect what the patient is actually taking, not just what the discharge summary says. Discrepancies between the hospital medication list and the medications in the home are common and must be documented and reconciled.
3. Incomplete functional scoring. The OASIS Section GG items require clinicians to score both the patient’s current performance and their discharge goals. Rushed scoring or scoring from memory after leaving the home leads to inaccurate baselines that suppress improvement scores at discharge.
4. Missing or vague medical necessity documentation. Medicare requires documentation that home health services are medically necessary and that the patient meets homebound criteria. A Start of Care assessment that does not clearly articulate this is vulnerable to denial on medical review.
5. Diagnosis sequencing errors. Under PDGM, the primary diagnosis drives the clinical grouping, which directly affects payment. An incorrect primary diagnosis at Start of Care means the wrong case-mix group and incorrect reimbursement for the entire 30-day period.
How to Improve Start of Care Documentation
Automate Referral Data Extraction
Roughly 30 percent of the data entered during a Start of Care already exists in the referral packet. Patient demographics, insurance information, diagnosis codes, medication lists, surgical history, and physician information are all sitting in documents that were faxed or electronically transmitted from the hospital or physician office.
AI-powered automation can read these documents and pre-populate the EMR before the clinician opens the chart. When the nurse arrives at the patient’s home, she verifies and confirms rather than typing from scratch. This eliminates 30 to 45 minutes of redundant data entry per admission.
Document at the Point of Care
Every minute between the clinical observation and the documentation entry is a minute of accuracy lost. Clinicians who complete OASIS scoring during the visit, while the patient is in front of them, produce more accurate assessments than those who finish hours later from memory.
Ambient documentation tools that capture clinical observations in real time can help clinicians stay present with the patient while ensuring the data is captured accurately. The goal is to close the chart before leaving the patient’s home.
Pre-Build the Chart Before the Visit
The Start of Care visit should not begin with a blank screen. Assign intake staff or use automation to load the referral data, draft the medication list, pull prior assessment data if the patient has been on service before, and confirm the visit logistics.
When the clinician opens the chart in the patient’s home, it should already be 30 to 40 percent complete. She is building on a foundation rather than starting from zero.
Standardize Narrative Templates by Diagnosis
Clinical narratives should not be composed from scratch every time. Build templates for your most common admission scenarios: CHF, wound care, joint replacement, COPD, and diabetes management.
Each template should prompt for the key clinical elements that Medicare expects to see: current status, functional impact, medical necessity justification, homebound rationale, and measurable goals. The clinician fills in the patient-specific details rather than structuring the entire narrative herself.
Validate Before Submission
QA rework is one of the biggest hidden time costs in home health. Charts that get returned for correction require the clinician to reopen a case she closed days ago, recall the details, and fix inconsistencies.
AI-powered validation can catch mismatches between OASIS scores and narrative documentation before the chart is submitted. Fixing an error at the point of care takes seconds. Fixing it three days later takes 15 minutes and often introduces new errors.
The Revenue Impact of Start of Care Accuracy
Start of Care documentation is not just a clinical exercise. It is a financial one.
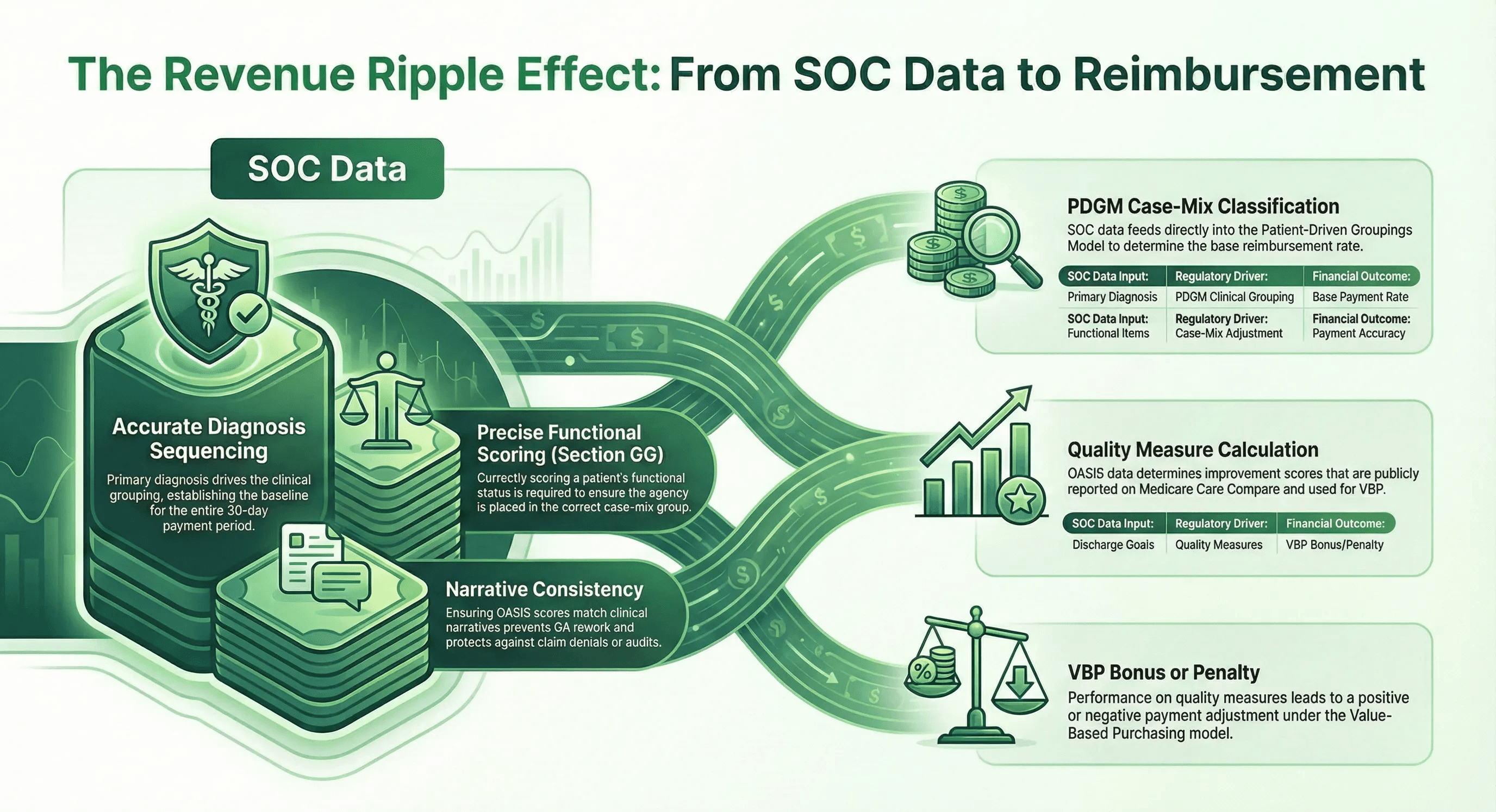
Under PDGM, the data entered at Start of Care determines the 30-day payment period’s case-mix classification. An inaccurate primary diagnosis, an incorrect functional score, or a missing comorbidity adjustment can result in underpayment for the entire episode. Multiply that across hundreds of admissions per year and the revenue impact is substantial.
Documentation accuracy at Start of Care also affects your agency’s performance in the Home Health Value-Based Purchasing Model. Quality measures derived from OASIS data, including functional improvement scores, directly influence your VBP payment adjustment. Agencies that score patients inaccurately at Start of Care may show artificially low improvement at discharge, which suppresses their quality scores and reduces their VBP bonus.
And the HHCAHPS patient satisfaction survey, which is being redesigned for April 2026, carries weight in both star ratings and the VBP model. When clinicians spend the majority of the visit staring at a screen rather than engaging with the patient, satisfaction scores decline.
Start of Care Under the All-Payer Mandate
Since July 1, 2025, CMS requires OASIS data collection and submission for all patients regardless of payer source. Every Medicare Advantage, Medicaid, commercial, self-pay, and even charity care patient who receives skilled services from a Medicare-certified home health agency now requires a full Start of Care OASIS.
For agencies where 30 to 50 percent of patients were previously exempt from OASIS, this represents a proportional increase in Start of Care documentation volume. The same nurses are performing more comprehensive assessments without additional time or staff.
This mandate makes documentation efficiency at Start of Care a survival issue, not a nice-to-have. The agencies absorbing the volume increase without burning out their workforce are the ones that automated the manual data entry before the mandate took effect.
Preparing for OASIS-E2
Effective April 1, 2026, CMS is implementing OASIS-E2, which includes several changes relevant to Start of Care documentation. The COVID-19 vaccination item (O0350) is being removed, the transportation item is being revised (new A1255 replacing A1250), and the skip pattern for M0102 has been modified.
While OASIS-E2 is a refinement rather than a major overhaul, agencies should coordinate with their EMR vendor on software updates and train clinicians on the changed items before the April 1 implementation date. Scrambling to learn new items while absorbing increased all-payer volume is a recipe for errors.
The Bottom Line
The Start of Care visit is where home health episodes succeed or fail. Every downstream assessment, every quality measure, every payment calculation, and every patient satisfaction score traces back to the data collected during this single visit.
The agencies that invest in making Start of Care documentation faster and more accurate, through pre-visit automation, point-of-care documentation, narrative templates, and real-time validation, will outperform the agencies that continue to rely on manual processes and after-hours charting.
Your clinicians did not choose this profession to spend their evenings typing. Give them the tools to close the chart before they leave the patient’s home.
Copper Digital builds AI agents that automate the intake and documentation workflow for home health agencies. We pre-populate Start of Care charts from referral data, validate OASIS accuracy before submission, and help your clinicians eliminate pajama time.
See how Copper AI transforms the Start of Care →

