Blog
Feb 6, 2026
Homebound Status Documentation: What Survives MAC Review

Arvind Sarin

Homebound status is the single most audited eligibility criterion in home health. It is the reason most ADRs get issued, the reason most medical review denials are upheld, and, when documented correctly, one of the most defensible findings in your chart. The gap between charts that survive MAC review and charts that get denied is rarely clinical. It is documentation precision.
The Medicare Benefit Policy Manual (Chapter 7, Section 30.1) defines homebound status in specific terms. MACs are not looking for clinical notes that describe a sick patient. They are looking for language that maps directly to that definition. When it is absent, vague, or copied from the previous visit, the denial follows.
This post covers what the definition actually requires, the most common documentation failures that MACs cite, and the specific language patterns that hold up under review.
What the Medicare Definition Actually Requires
The homebound definition in the Medicare Benefit Policy Manual, Chapter 7, §30.1, requires documentation of two conditions. Not just one.
Condition 1: Leaving the home requires a considerable and taxing effort.
The patient must have a condition, whether due to illness, injury or a psychiatric condition, that restricts their ability to leave home. The effort required to leave must be considerable and taxing. Normal fatigue does not meet this standard. Shortness of breath with ambulation, pain with weight-bearing, fall risk requiring assistance, or post-surgical mobility restriction do.
Condition 2: The patient is either unable to leave or only leaves infrequently or for absences of short duration.
Leaving home occasionally does not disqualify a patient from homebound status, but the nature and frequency of absences must be documented. Leaving for medical appointments, adult day programs, or rare family events is permissible. Leaving daily, driving independently, or working outside the home is not.
DEFINITION NOTE: A patient can be homebound and still leave the home. The key documentation requirement is that leaving requires considerable and taxing effort, and any absences outside the home are infrequent or of short duration. Both conditions must be present in the chart. |
What MACs Actually Look for in a Homebound Determination
MACs reviewing homebound status are not reading clinical notes for general clinical detail. They are scanning for specific documentation elements. In published Local Coverage Determinations and ADR guidance, the following elements appear consistently as required.
The specific condition causing the restriction
Generic statements like "patient is weak" or "patient is elderly" do not meet the standard. The note must identify the underlying diagnosis or condition: CHF with dyspnea on minimal exertion, bilateral lower extremity weakness post-stroke, or a stage III wound preventing weight-bearing. The condition must be linked to the mobility restriction.
The functional consequence that makes leaving taxing
What specifically happens when the patient attempts to leave the home? Can they ambulate to the car without becoming short of breath? Can they transfer independently? Do they require assistance from another person, a device, or both? The note must describe the functional limitation, not just the diagnosis.
What would leaving the home require
Does the patient need another person present to leave safely? Do they require a wheelchair, walker, or other assistive device? Does the level of effort involved, even with assistance, constitute a considerable taxing effort? This is the bridge between the clinical finding and the statutory definition.
Absences from the home: what they were for and how often
If the patient leaves the home at all, the frequency and reason must be documented. "Patient leaves only for medical appointments" is a commonly used phrase and is legally sufficient when it accurately reflects the patient's situation. What is not sufficient: leaving the reason blank, leaving the frequency blank, or failing to document absences that the patient later discloses.
MAC AUDIT PATTERN One of the most common audit findings is inconsistency between what the patient reports in OASIS M1033 (Risk for Hospitalization) and what appears in the homebound narrative. If a patient reports driving to appointments in the OASIS and the visit note says the patient is unable to leave independently, the record is internally inconsistent. That inconsistency is very difficult to defend. |
The Most Common Documentation Failures That Cause Denials
Based on published MAC denial patterns and OIG audit findings, these are the documentation failures most frequently cited as the basis for homebound status denials.
1. Using the same boilerplate language on every visit
Copy-forward documentation, where the homebound narrative is identical across every visit note, is a red flag in any MAC review. It suggests the determination was never actually reassessed. Reviewers will note identical language across 10 or 20 visit dates and treat the documentation as unreliable.
The fix is not an elaborate variation. It is documentation that reflects what actually changed. If the patient's functional status was the same, say so and explain why leaving remains taxing. If it changed, document how.
2. Vague functional language without specificity
Phrases that fail MAC review on their own: "patient is weak", "patient is deconditioned", "patient has difficulty ambulating", "patient has limited mobility." None of these connect a specific clinical finding to the statutory standard.
Phrases that survive review: "Patient ambulates 10 feet with rolling walker, requires maximum assist for transfers, becomes short of breath at rest after any exertion. Leaving the home would require ambulance transport and poses a significant safety risk."
3. Failure to document homebound status on every visit note
Homebound status must be re-established on every visit. It cannot be assumed from the SOC certification. MACs reviewing an episode will look at every visit note. If homebound status is absent from 8 of 12 visit notes, the documentation does not support the entire episode, even if the SOC and recertification notes are solid.
4. Inconsistency with OASIS functional items
OASIS functional items, particularly M1800 (Grooming), M1810/M1820 (Dressing), M1840 (Toilet Transferring), M1850 (Transferring), and M1860 (Ambulation/Locomotion), create a functional profile that reviewers cross-reference against homebound narratives. If a patient is scored as independent on M1860 and the visit note claims the patient cannot safely ambulate outside the home, the inconsistency will be flagged.
5. Not documenting what leaving the home would require
Many clinicians document what the patient cannot do, but skip documenting what leaving the home would actually require. The regulatory standard is about effort and burden, not absolute inability. "Patient can leave the home only if transported by wheelchair-accessible vehicle with two-person assist" is stronger documentation than "patient is non-ambulatory."
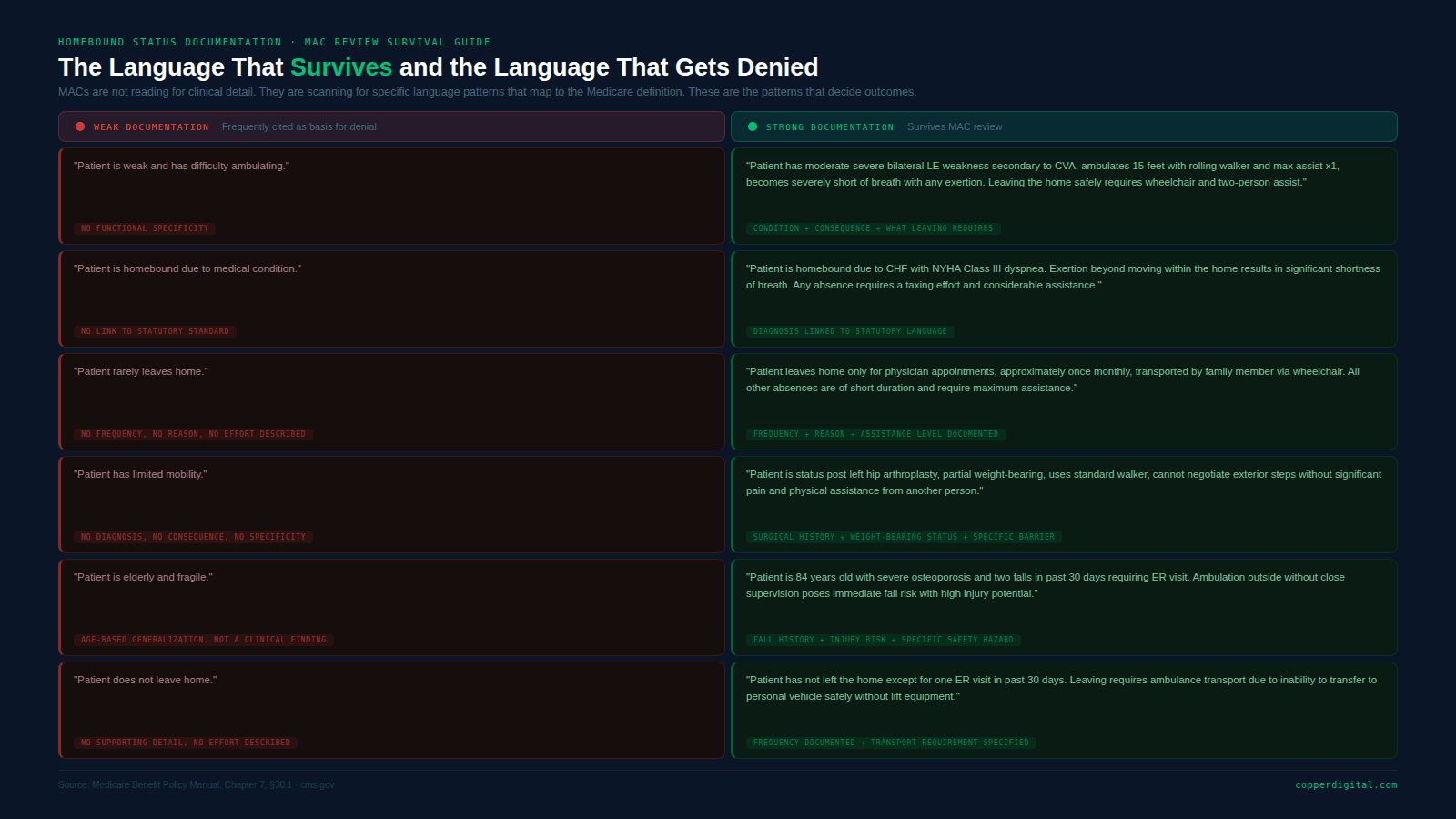
Homebound Documentation: Weak vs. Strong Language Patterns
The following table shows the types of documentation patterns that appear in denied claims versus the documentation patterns that survive review. These are not invented examples. They reflect language patterns cited in published CMS and OIG guidance.
What a MAC Reviewer Checks in the First 60 Seconds
Understanding how a MAC reviewer works through a chart helps agencies understand which documentation elements carry the most weight early in a review.
Step 1: SOC OASIS and Face-to-Face Documentation.
The reviewer will check whether the face-to-face encounter note contains a statement that homebound status was assessed and met at the time of the encounter. The physician's narrative must support homebound status. It cannot simply state the diagnosis. Per CMS guidance, the face-to-face encounter note is not the same as the physician certification and must stand on its own.
Step 2: OASIS Functional Items.
The reviewer will scan M1850 (Transferring) and M1860 (Ambulation/Locomotion) against the homebound narrative in the SOC visit note. If those items show a patient who is independent or requires setup assist only, the homebound claim is likely to be challenged unless the narrative explains why leaving the home is still taxing despite those functional scores.
Step 3: Visit Notes for Consistency.
The reviewer will sample visit notes, typically 3 to 5, looking for homebound language. Absent: the note fails. Present but identical across all visits: treated as unreliable. Present and specific to the current visit: the patient's current functional status with specific detail, it holds.
Step 4: Recertification OASIS.
At recertification, the homebound status must be re-established. If the patient has improved functionally, as measured by OASIS items, but remains on service, the recertification documentation must explain why homebound criteria are still met despite functional gains.
CLINICAL INSIGHT A patient can show functional improvement on OASIS and remain homebound. The clinical documentation must explain the disconnect. Example: "Patient has improved transfers from max assist to moderate assist but continues to require two-person assist to safely navigate exterior steps and enter a vehicle. Leaving the home remains a taxing effort requiring assistance." |
Psychiatric Homebound Status: A Separate Documentation Standard
Patients can qualify as homebound on psychiatric grounds under 42 CFR §409.42(a) if leaving home would have a medically documented adverse effect on the patient's psychiatric condition. This is a separate pathway that many agencies document inadequately.
For psychiatric homebound status to survive MAC review, the chart must contain:
A specific psychiatric diagnosis, not a behavioral descriptor
A documented statement from the treating clinician (or psychiatric evaluator) that leaving the home would exacerbate the patient's condition
Documentation of what specifically about leaving home triggers the adverse effect: agoraphobia, severe anxiety disorder, and psychotic symptoms worsened by external stimuli
Evidence that the treating physician concurs with the homebound determination on psychiatric grounds
Generic statements such as "the patient has anxiety and does not leave home" do not meet the standard. The psychiatric homebound pathway requires the same level of clinical specificity as the physical homebound pathway.
How Automation Changes the Homebound Documentation Problem
The two biggest homebound documentation failures, copy-forward language and missing homebound statements on visit notes, are both documentation workflow problems. They occur because clinicians are documenting after the visit, under time pressure, using free-text fields that have no structure or guardrails.
Agencies that have moved to structured homebound documentation workflows report fewer ADRs on homebound grounds. The structure varies, but the common elements are:
Guided homebound prompts at documentation time. The clinician is asked at each visit: what is the condition causing the restriction, what would leaving the home require, and how often does the patient leave. The answers populate the homebound narrative rather than the clinician writing free-text from memory.
OASIS cross-reference. The homebound narrative is checked against M1850 and M1860 before the visit note is finalized. If the patient is scored as independent on ambulation but the homebound narrative claims ambulatory dependence, the inconsistency is flagged before the chart is submitted.
Visit-level completeness check. Every visit note is reviewed before finalization for the presence of a homebound statement. Notes without one are flagged for completion.
Pre-audit homebound audit trail. At the point of MAC review or ADR, the agency can pull a report showing homebound documentation across all visit notes for the episode: consistent, specific, and current as of each visit date.
Copper Digital's OASIS documentation automation includes structured homebound documentation workflows that guide clinicians through each element of the regulatory standard at the point of care, cross-reference against OASIS functional scores, and flag missing or inconsistent documentation before the chart is finalized.
Homebound Documentation Quick Reference
Every visit note that involves homebound status should be able to answer all of the following:
Required Documentation Element | Where It Appears in the Chart |
|---|---|
Specific diagnosis or condition causing the restriction | SOC visit note, recertification note, and every visit note |
Functional consequence of the condition (what happens when the patient attempts to leave) | Every visit note. Must be specific, not generic |
What leaving the home would physically require (person, device, transport) | Every visit note |
Frequency of any absences from home and the reason for each | Every visit note, if applicable |
Physician face-to-face encounter note supporting homebound status | F2F documentation, separate from the certification |
Consistency between OASIS functional items and homebound narrative | OASIS items M1850, M1860 cross-referenced to visit note |
Recertification homebound re-establishment with updated functional status | Recertification OASIS and visit note |
Frequently Asked Questions
Can a patient be homebound if they leave home for medical appointments?
Yes. The Medicare Benefit Policy Manual explicitly states that leaving home for the purpose of receiving medical treatment is not inconsistent with homebound status. Leaving for adult day programs approved under Medicare is also permissible. What the documentation must reflect is that the patient only leaves infrequently, for brief durations, or for medical purposes, and that leaving requires a considerable and taxing effort.
Does homebound status need to be documented on every visit note?
Yes. MACs reviewing an episode will examine every visit note. Homebound status must be re-established at each visit. It is not sufficient to document it only at SOC and recertification. The visit note must contain language specific to that visit date that supports the homebound determination.
What is the difference between the face-to-face encounter note and the physician certification?
The physician certification is the physician's attestation that the patient requires home health services and is homebound. The face-to-face encounter note is the clinical documentation of the encounter that occurred within 90 days before or 30 days after the start of care. The face-to-face note must contain a physician narrative, not just a diagnosis code, that supports homebound status. CMS has clarified that rubber-stamped or checkbox face-to-face notes do not meet the documentation standard.
Can a patient who has improved functionally still be homebound?
Yes. Functional improvement does not automatically disqualify homebound status. The documentation at recertification must explain why the patient continues to meet the homebound standard despite functional gains. For example, a patient who has improved from maximum assist to moderate assist for transfers may still require two-person assist to safely navigate exterior stairs and enter a vehicle, which can still constitute a considerable and taxing effort.
What triggers a MAC ADR for homebound status?
Several patterns are known to trigger ADRs on homebound grounds: billing patterns that differ significantly from peers in the same region (flagged through PEPPER reports), patients with functional OASIS scores inconsistent with homebound status, high episode volume from a single referral source, and agencies identified through prior authorization or targeted probe and educate (TPE) programs. The strongest defense against any ADR is complete, specific, and consistent homebound documentation from SOC through discharge.
GET AUDIT-READY HOMEBOUND DOCUMENTATION Copper Digital's OASIS documentation automation guides clinicians through structured homebound documentation at every visit, with built-in cross-checks against OASIS functional scores and completeness flags before the note is finalized. |
Related Reading
Sources

