Blog
Jan 15, 2026
How to Reduce OASIS Documentation Time in Home Health

Arvind Sarin

Your nurses did not go to school for data entry. But that is how most of them spend their day.
The average home health clinician spends more time documenting a visit than performing it. Start of Care assessments routinely consume four to six hours of total labor, even though the scheduled visit is only two. Recertifications are not much better. Routine visits stack up. By the end of the week, your best nurses are buried in screens instead of sitting with patients.
This is not a motivation problem. It is a workflow problem. And it has a fix.
Here is a practical breakdown of where OASIS documentation time actually goes, and how to take it back.
Where the Time Goes
Before you can reduce documentation time, you need to see where it disappears.
Most agencies assume the bottleneck is the OASIS assessment itself. It is not. The bottleneck is everything surrounding it: pre-visit preparation, redundant data entry, post-visit charting, and QA rework.
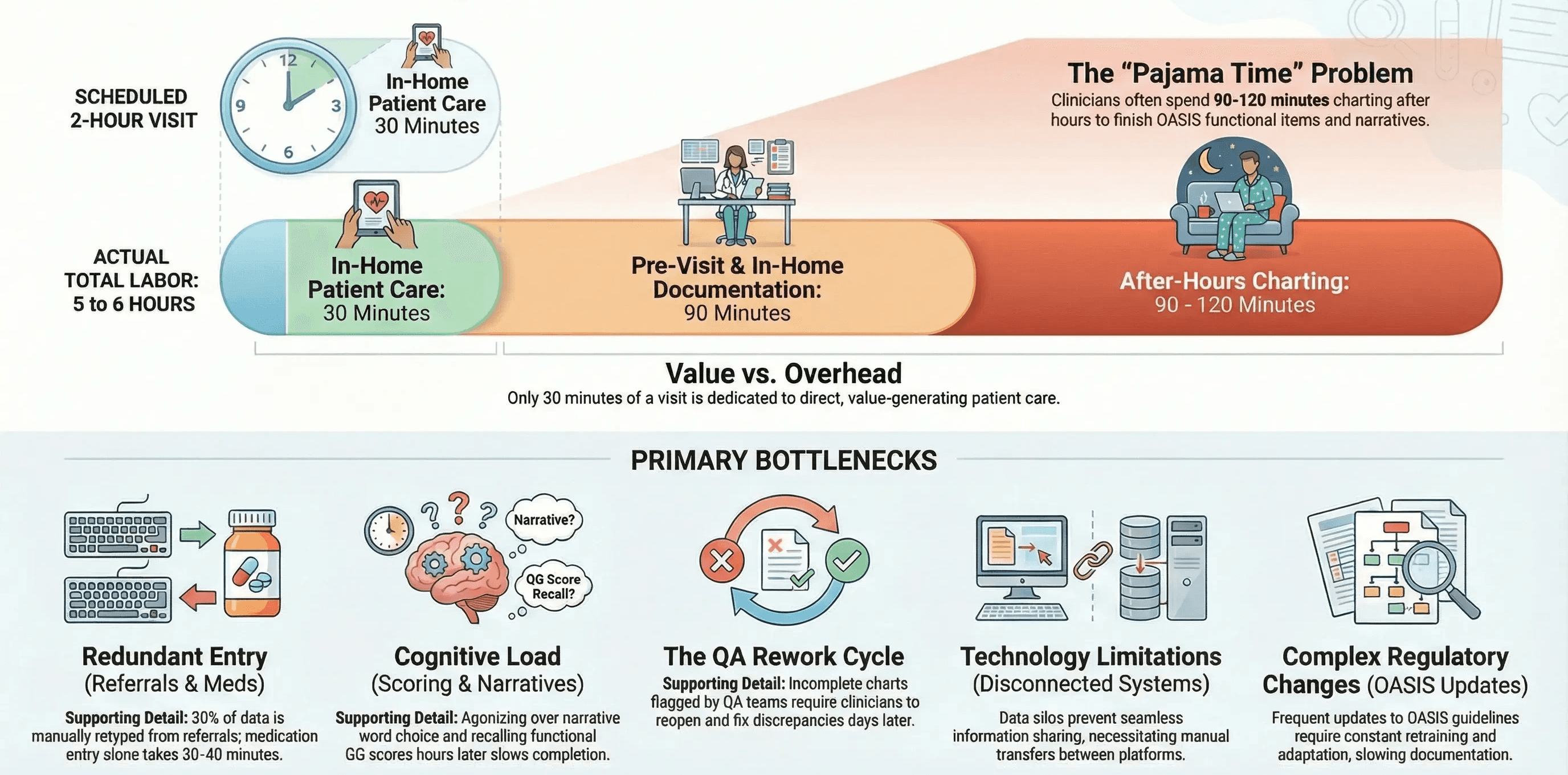
Here is a realistic breakdown of how a single Start of Care visit plays out:
Pre-visit preparation (30 minutes). The clinician reviews the referral packet, deciphers faxed hospital notes, confirms the patient's address, and maps the route. Most of this time is spent manually extracting information that already exists in a PDF.
In-home patient care (30 minutes). This is the actual clinical work: listening to heart sounds, assessing wounds, educating the patient, and reviewing medications face-to-face. This is the only part of the visit that directly generates value.
In-home documentation (60 minutes). The clinician sits at the dining table, clicking through OASIS fields, hunting for diagnosis codes, and typing narrative notes. The patient waits. The connection between nurse and patient dissolves into screen time.
After-hours charting (90-120 minutes). The nurse leaves the home with a chart that is only partially complete. After dinner, she opens her laptop. She finishes the OASIS functional items, cross-references the medication profile, writes outcome goals, and reconciles the clinical narrative.
That is roughly five to six hours of labor for a visit that was scheduled for two.
The problem scales. An agency running 20 admissions per week is losing over 60 hours of clinician time to documentation overhead alone. That is more than one full-time employee doing nothing but paperwork.
The 5 Biggest Time Drains in OASIS Documentation
Not all documentation tasks are equal. Some consume disproportionate time for the value they produce. These are the five areas where most agencies lose the most hours.
1. Redundant Data Entry from Referral Documents
Roughly 30 percent of the data your clinician types during a Start of Care already exists somewhere else. The patient's name, date of birth, address, insurance ID, primary diagnosis, surgical history, and medication list are sitting in the referral packet from the hospital or physician's office.
Yet we ask nurses to retype this information into the EMR manually.
This is the single largest time drain in home health documentation. It is also the most solvable. The information does not need to be generated. It needs to be transferred. The U.S. Surgeon General’s advisory on health worker burnout specifically calls out administrative burdens as a primary driver of workforce exhaustion. Redundant data entry is one of the clearest examples.
2. Medication Reconciliation
The average home health patient takes 13 medications. Manually entering each one, including the drug name, dosage, route, frequency, and prescribing physician, takes approximately 1.5 minutes per medication. That is 20 minutes per patient on medication entry alone.
When you factor in cross-referencing the hospital discharge summary against what the patient actually has in the home, the real number is closer to 30 to 40 minutes.
3. OASIS Functional Scoring
The OASIS GG items require clinicians to score the patient’s functional abilities across multiple categories: self-care, mobility, transfers, and more. Each item requires the clinician to observe or assess, select the correct score, and document a supporting narrative.
The challenge is not complexity. The challenge is that clinicians often complete these items hours after leaving the patient’s home, relying on memory rather than real-time observation. This slows the process and introduces inaccuracy.
4. Clinical Narrative Writing
Medicare requires that the clinical record tell a coherent story. The narrative must explain why skilled care is medically necessary, connect the diagnosis to the functional deficits, and justify the plan of care.
Most clinicians are excellent at delivering care. Fewer are comfortable writing narratives that satisfy an auditor. The result is time spent agonizing over word choice, second-guessing phrasing, and rewriting paragraphs that do not quite connect.
5. QA Rework and Returned Charts
Incomplete or inconsistent documentation does not just disappear. It comes back. QA teams flag OASIS items that do not match the narrative. Charts get returned for correction. The clinician has to reopen a chart she closed days ago, recall the details, and fix the discrepancies.
This cycle of submission, rejection, and rework adds hours to every episode of care and is one of the top contributors to clinician frustration.
7 Strategies to Reduce OASIS Documentation Time
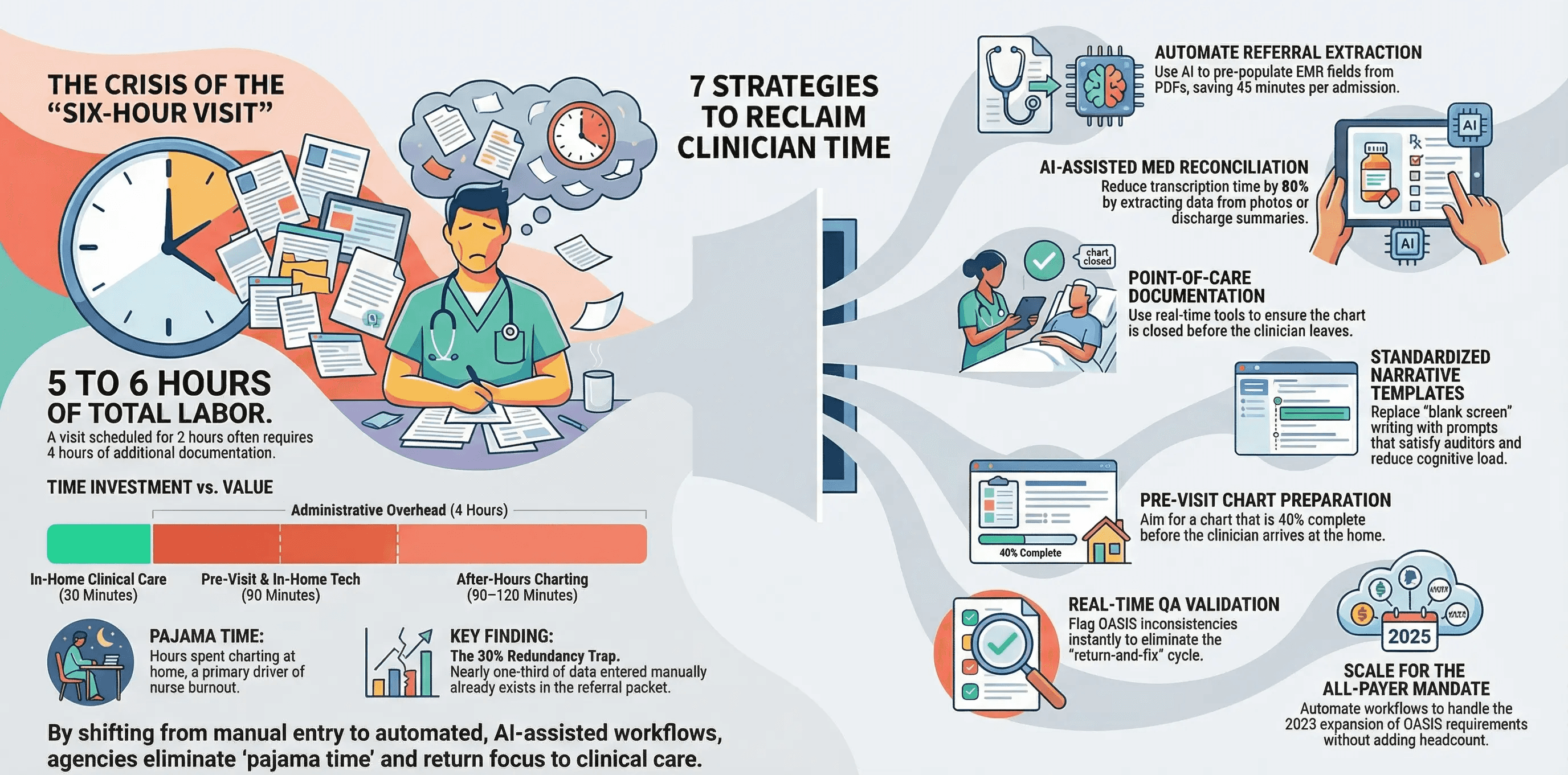
Strategy 1: Automate Referral Data Extraction
The highest-impact change you can make is to stop asking nurses to type information that already exists in writing.
AI-powered intake automation can read raw referral documents, hospital discharge summaries, and physician orders. It extracts patient demographics, diagnosis codes, medication lists, surgical history, and insurance information. It then pre-populates those fields in the EMR before the clinician ever opens the chart.
When the nurse arrives at the home, she is verifying data instead of entering it. This alone can eliminate 30 to 45 minutes of manual entry per admission.
Strategy 2: Use AI-Assisted Medication Reconciliation
Instead of manually typing 13 medications from a discharge summary, technology can extract medication data from referral documents, photos of pill bottles, and handwritten medication lists.
The clinician reviews and confirms. She does not transcribe.
Early adopters of AI medication reconciliation report 60 to 80 percent reductions in time spent on this single task.
Strategy 3: Document at the Point of Care
Every minute of documentation delayed is a minute of accuracy lost. When a clinician completes OASIS scoring three hours after leaving the home, she is working from memory. Memory is unreliable.
Encourage real-time documentation during the visit. Better yet, use ambient documentation tools that capture clinical observations as they happen, so the clinician can stay focused on the patient.
The goal is zero after-hours charting. Every visit should be closed before the clinician moves to the next. The American Medical Association has termed this after-hours documentation problem “pajama time,” and it remains one of the most cited drivers of clinician dissatisfaction.
Strategy 4: Standardize Clinical Narrative Templates
Clinical narratives should not be written from scratch every time. Build narrative templates that align with your most common diagnoses and care scenarios.
A CHF admission narrative template should prompt for key elements: current weight, edema status, medication compliance, dietary education provided, and functional impact. The clinician fills in the patient-specific details rather than composing an essay.
Templates do not replace clinical judgment. They reduce the cognitive burden of structuring the documentation.
Strategy 5: Implement Pre-Visit Chart Preparation
Assign a staff member or use automation to prepare the chart before the visit. This means the referral data is loaded, the medication list is drafted, prior OASIS scores are referenced, and the visit schedule is confirmed.
When the clinician sits down in the patient’s home, the chart should already be 30 to 40 percent complete. She is building on a foundation rather than starting from a blank screen.
Strategy 6: Reduce QA Rework with Real-Time Validation
QA rework is a downstream symptom of upstream documentation gaps. If you catch inconsistencies before the chart is submitted, you eliminate the return-and-fix cycle entirely.
AI-powered validation can flag mismatches between OASIS scores and clinical narratives in real time. If the functional score says the patient is independent in bathing, but the narrative describes moderate assistance, the system flags it before submission.
Fixing a discrepancy at the point of documentation takes 30 seconds. Fixing it three days later takes 15 minutes.
Strategy 7: Align OASIS Scoring with the All-Payer Mandate
Since July 2025, CMS requires all-payer OASIS data collection and submission for all patients regardless of payer source. This means your documentation burden has expanded significantly. Every Medicare Advantage, Medicaid, commercial, and even self-pay patient now requires full OASIS completion.
If you have not already optimized your OASIS workflow, this mandate makes it urgent. The agencies that are handling the expanded volume without adding headcount are the ones that invested in automation before the mandate hit.
With OASIS-E2 changes taking effect in April 2026 and a redesigned HHCAHPS survey on the horizon, documentation demands will continue to grow. Manual processes cannot scale to meet them.
The Real Cost of Doing Nothing
Documentation burden is not just a time problem. It is a staffing problem, a revenue problem, and a patient satisfaction problem.
Clinicians who spend their evenings charting burn out faster. The National Academy of Medicine found that burnout had reached crisis levels among the U.S. health workforce even before the pandemic. Agencies with a high documentation burden report higher turnover. Replacing a single home health nurse costs between $30,000 and $60,000 when you factor in recruiting, onboarding, and lost productivity.
Slow documentation also delays billing. Every day between the visit and the submitted claim is a day your cash flow is frozen. Agencies that close charts on the same day as the visit see measurably faster reimbursement cycles.
And patients notice. When a nurse spends 60 minutes of a two-hour visit staring at a screen, the patient does not feel cared for. They feel processed. This shows up directly in HHCAHPS satisfaction scores, which now feed into Value-Based Purchasing calculations that affect your reimbursement.
Start With the Biggest Lever
You do not have to fix everything at once. Start with the change that produces the most immediate time savings.
For most agencies, that is referral data extraction and pre-visit chart preparation. This is the step that eliminates the largest block of redundant manual work without changing anything about how your clinicians practice.
Copper Digital builds AI agents specifically for this problem. Our platform reads referral documents, extracts the data, and pre-populates the chart before your nurse opens it. No new hardware. No change to your EMR. Just less typing and more time for patient care.
See how Copper AI reduces OASIS documentation time →

