Blog
Apr 22, 2026
Medicare Advantage in Home Health: Prior Auth, Lower Reimbursement, and How to Survive It

Arvind Sarin, CEO& Chairman of Copper Digital

If your agency's payer mix looks anything like the national average, more than half of your Medicare patients are now in Medicare Advantage plans. That number has been growing steadily for a decade, and the trend is accelerating. According to CMS data, MA enrollment has crossed 33 million beneficiaries, representing over 54% of all Medicare-eligible individuals. For home health agencies that built their operations around Traditional Medicare's fee-for-service model, this is not an incremental change. It is a structural shift in how you get paid, how quickly you get paid, and how much work you have to do to get paid at all.
We hear from agency owners every week who are feeling the pressure. Their margins are thinning. Their billing teams are spending more time on authorizations and appeals than on actual claims processing. Their nurses are seeing the same patients but generating less revenue per episode. And their referral sources are sending patients whose coverage comes with strings that Traditional Medicare never had. The operational model that worked when 80% of your patients were fee-for-service does not work when 60% are MA.
What Medicare Advantage Actually Changes for Home Health
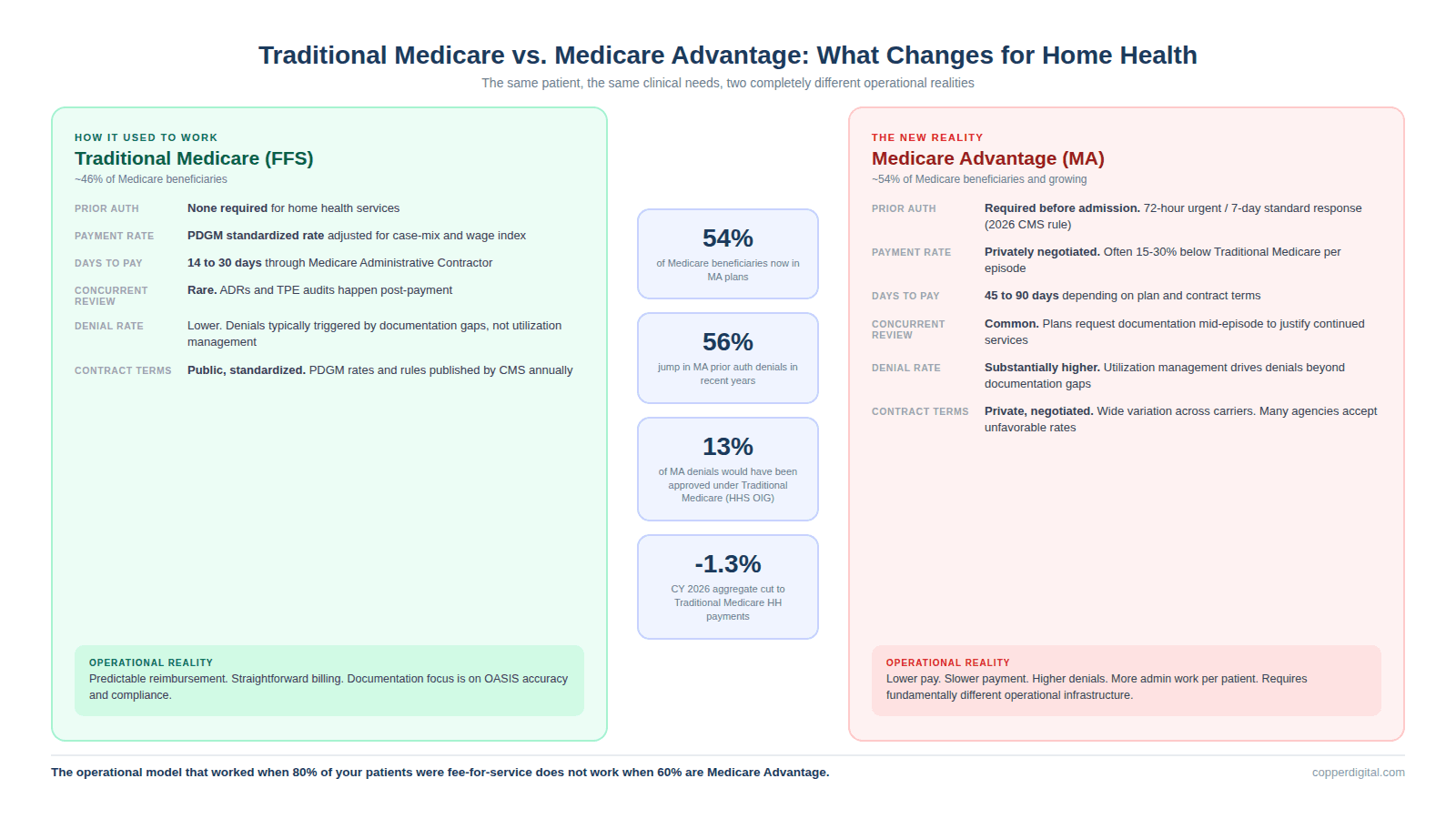
Traditional Medicare pays home health agencies under the Prospective Payment System using PDGM, which assigns a case-mix weight to each 30-day episode based on clinical characteristics, functional impairment level, and comorbidity adjustments. The rate is standardized nationally and adjusted for wage index. You submit your OASIS data, your claim goes through the Medicare Administrative Contractor, and in most cases, payment arrives within 14 to 30 days. There is no prior authorization requirement for home health services under Traditional Medicare.
Medicare Advantage changes nearly every part of that process. MA plans are private insurers that contract with CMS to provide Medicare benefits. They are permitted to use utilization management tools including prior authorization, concurrent review, and retrospective review. They set their own reimbursement rates, which are often lower than Traditional Medicare. They can require documentation beyond what CMS mandates. And they control the payment timeline, which frequently stretches to 45, 60, or 90 days depending on the plan and your contract terms.
The practical impact on an agency is significant. You now have to obtain authorization before admitting a patient, which adds time to the intake process and delays the start of care. You have to manage concurrent reviews where the plan requests additional documentation mid-episode to justify continued services. You have to track authorization windows, because if the authorization expires before the episode ends, you are providing care without coverage. And you have to build an appeals infrastructure, because MA denial rates are substantially higher than Traditional Medicare denial rates.
The Prior Authorization Problem Is Getting Worse, Not Better
Prior authorization denials in Medicare Advantage jumped 56% in recent years according to industry reporting. A 2022 HHS Office of Inspector General report found that 13% of prior authorization requests denied by MA plans would have been approved under Traditional Medicare's coverage rules. The same report found that 18% of payment requests denied by MA plans met standard Medicare coverage and billing rules. That means MA plans are denying claims that Traditional Medicare would have paid, and the burden of proving the plan wrong falls entirely on the agency.
The American Hospital Association has documented that MA prior authorization practices are delaying hospital discharges and causing capacity issues for acute care hospitals, which directly affects home health referral flow. When a hospital cannot discharge a patient because the MA plan has not approved home health services, the referral sits in limbo. The agency cannot schedule the SOC visit. The nurse cannot be assigned. The 48-hour timely initiation clock is ticking against a process the agency does not control. AHA's comment letter on the CY 2026 Home Health PPS rule specifically called out MA prior authorization as a systemic barrier to care access.
CMS has taken steps to address this. The CMS Interoperability and Prior Authorization Final Rule, which took effect January 1, 2026, requires MA plans to respond to expedited prior authorization requests within 72 hours and standard requests within 7 calendar days. Plans must now provide a specific reason for every denial. They must publicly report their approval and denial rates. And they can no longer retroactively deny previously approved inpatient admissions except in cases of fraud or obvious error. These are meaningful improvements. But they do not change the fundamental reality that agencies are still responsible for submitting authorizations, tracking responses, managing concurrent reviews, and filing appeals. The administrative work has not gone away. It has gotten a regulatory framework around it.
Lower Reimbursement Is Compounding the Problem
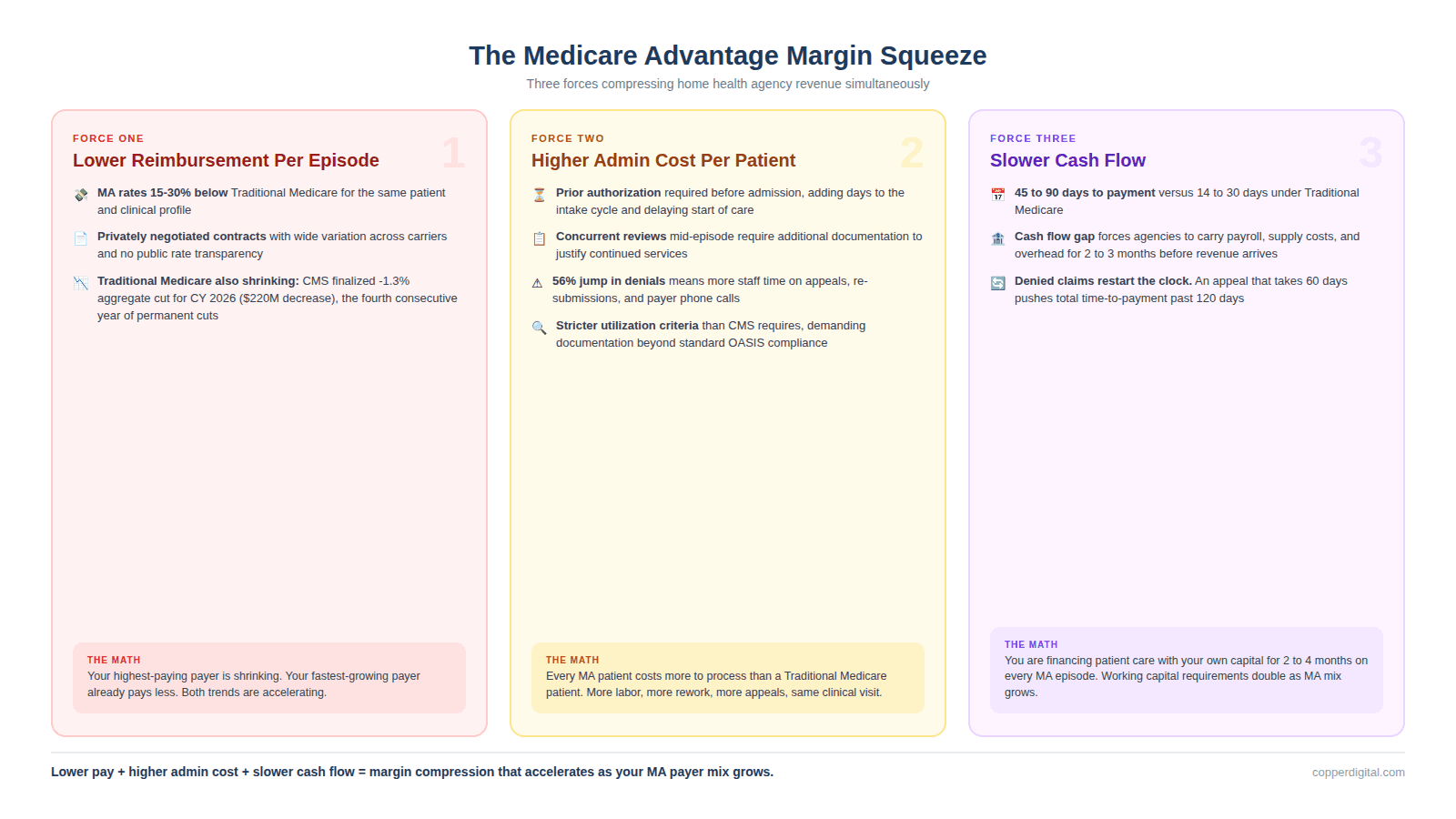
MA reimbursement for home health episodes is frequently lower than what Traditional Medicare pays for the same patient with the same clinical profile. The exact rates depend on your contract with each plan, and agencies report wide variation across carriers. Some plans pay rates comparable to Traditional Medicare. Others pay 15% to 30% less per episode. And unlike Traditional Medicare, where PDGM case-mix weights are transparent and publicly available, MA contracts are negotiated privately, and many agencies accept unfavorable rates because the alternative is losing access to a growing patient population.
This is happening against a backdrop of continuous cuts to Traditional Medicare home health payments. CMS finalized a 1.3% aggregate reduction in home health payments for CY 2026, representing approximately $220 million in decreased payments compared to 2025. This is the fourth consecutive year of permanent cuts to home health Medicare payments. While the final rule was less severe than the initially proposed 6.4% aggregate reduction, it still means agencies are earning less per episode on their Traditional Medicare patients while simultaneously managing lower-paying MA patients with higher administrative requirements.
The math is straightforward and uncomfortable. Your Traditional Medicare reimbursement is shrinking. Your MA reimbursement was already lower. Your administrative cost per MA patient is higher because of prior auth, concurrent review, and appeals. And the proportion of your patients on MA is growing every quarter. Without operational changes, the margin compression will continue until it crosses the line from tight to unsustainable.
What Your Operations Need to Survive an MA-Dominant Payer Mix
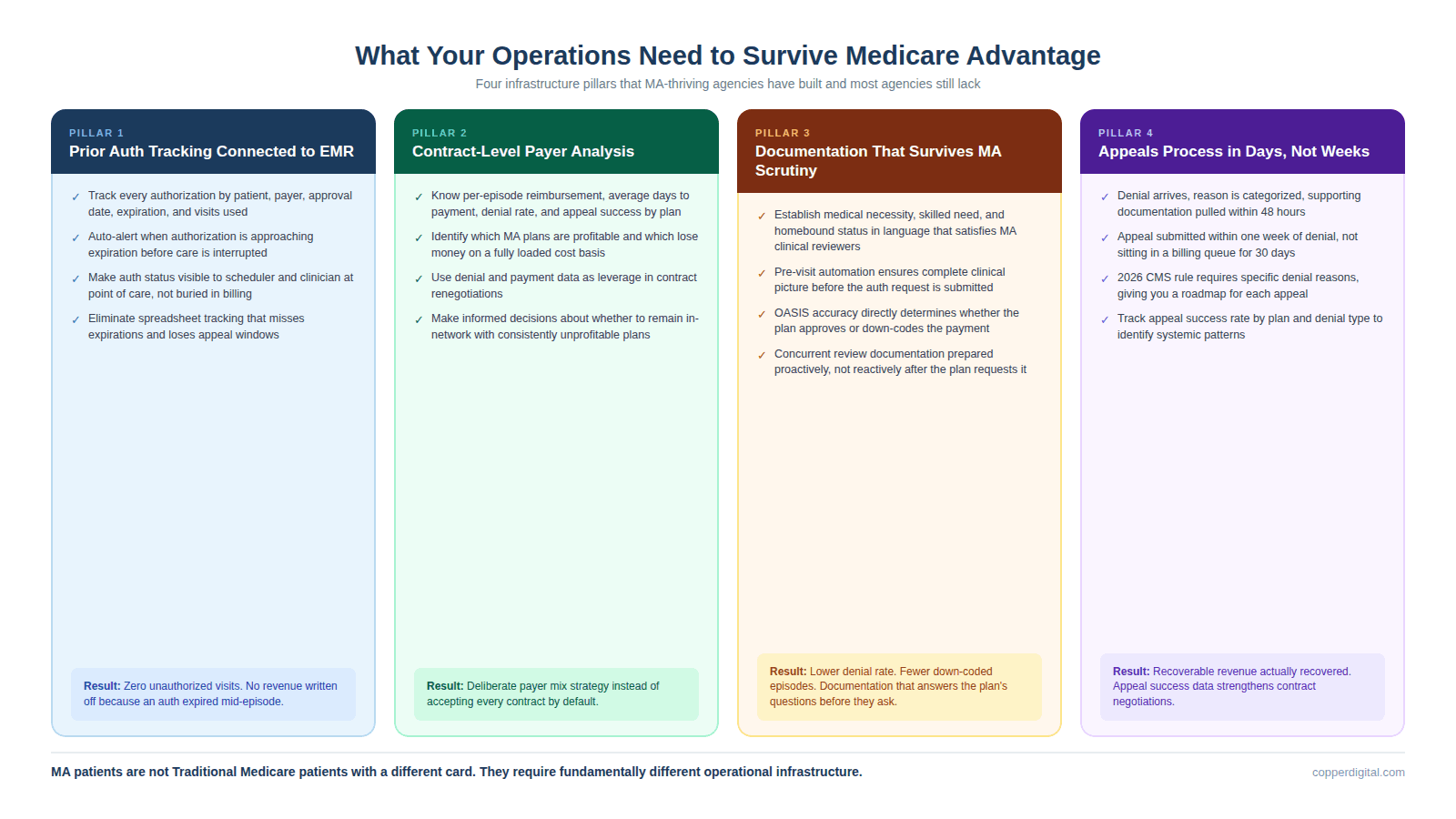
Agencies that are managing the MA transition well have built specific operational infrastructure that most agencies still lack. None of it is optional anymore.
Prior Authorization Tracking That Is Not a Spreadsheet
If your team is tracking prior authorizations in a shared spreadsheet or a Word document, you are going to miss expirations, lose appeals windows, and provide unauthorized care that will not be reimbursed. You need a system that tracks every authorization by patient, payer, approval date, expiration date, number of authorized visits, and visits used. The system needs to generate alerts when an authorization is approaching expiration so your team can submit a re-authorization request before care is interrupted. Agencies using Copper Digital's automation layer have connected this tracking directly to their EMR so that authorization status is visible to the scheduler and the clinician at the point of care, not buried in a billing department queue.
Contract-Level Payer Analysis
You need to know exactly what each MA plan pays you per episode, what the average days to payment is, what the denial rate is, and what the appeal success rate is, broken out by plan. Most agencies know their blended average but cannot tell you which plans are profitable and which are losing them money on a per-episode basis. That analysis should drive your contract negotiations, your payer mix strategy, and in some cases, your decision about whether to remain in-network with a specific plan. If a plan pays 25% less than Traditional Medicare, denies 30% of your claims, and takes 75 days to pay, you need to understand the fully loaded cost of serving that plan's patients before you accept the next referral.
Documentation That Survives MA Scrutiny
MA plans apply utilization management criteria that are often stricter than Traditional Medicare's coverage rules. Your documentation has to clearly establish medical necessity, skilled need, and homebound status in language that satisfies the plan's clinical reviewers, not just CMS. This is where the connection to OASIS accuracy and clinical documentation quality becomes a financial survival issue, not just a compliance issue. If your OASIS does not clearly support the functional impairment level that drives your case-mix weight, the MA plan will either deny the authorization or down-code the payment. Pre-visit automation that extracts referral data and pre-populates clinical documentation helps because it ensures the clinical picture is complete before the authorization request is submitted, not after the denial comes back.
An Appeals Process That Runs in Days, Not Weeks
Under the new CMS rules, MA plans must provide a specific reason for every denial. That reason becomes your roadmap for the appeal. But you have to act fast. Appeal windows are short, often 60 days for standard reconsideration. And many agencies let denials sit in a queue because the billing team is overwhelmed with routine claims processing. The agencies winning appeals have a dedicated workflow: denial comes in, reason is categorized, supporting documentation is pulled within 48 hours, and the appeal is submitted within a week. If your appeals process is slower than that, you are leaving recoverable revenue on the table.
The Strategic Question Nobody Wants to Ask
At some point, every agency owner has to answer a question that the industry does not like to discuss openly: Should I accept every MA plan, or should I be selective about which plans I contract with?
There is no universal answer. It depends on your market, your payer mix, your referral sources, and your margins. But the agencies that are thriving rather than just surviving in an MA-dominant environment are the ones that have done the math by plan and made deliberate decisions about which contracts make operational and financial sense. Some have exited plans that consistently pay below cost. Others have renegotiated rates using denial data and payment timing data as leverage. Others have built MA-specific documentation workflows that reduce the administrative cost enough to make marginal plans viable.
What none of the thriving agencies have done is continue operating as if MA patients are the same as Traditional Medicare patients. They are not. The payer expects different documentation. The authorization process requires different staffing. The payment timeline requires different cash flow planning. And the denial rate requires a different approach to revenue cycle management. Agencies that recognize this and build for it will grow. Agencies that do not will watch their margins erode until the math stops working.
Frequently Asked Questions
What is the difference between Medicare Advantage and Traditional Medicare for home health?
Traditional Medicare pays home health agencies under the Prospective Payment System using PDGM case-mix weights, requires no prior authorization for home health services, and typically pays within 14 to 30 days. Medicare Advantage plans are private insurers that contract with CMS. They can require prior authorization before admitting patients, apply concurrent and retrospective reviews, set their own reimbursement rates (often lower than Traditional Medicare), and control payment timelines that frequently extend to 45, 60, or 90 days. More than 54% of Medicare beneficiaries are now enrolled in MA plans, making this the dominant payer for most home health agencies.
How do new 2026 CMS rules affect Medicare Advantage prior authorization?
The CMS Interoperability and Prior Authorization Final Rule, effective January 1, 2026, requires MA plans to respond to expedited prior authorization requests within 72 hours and standard requests within 7 calendar days. Plans must provide a specific reason for every denial and must publicly report their approval and denial rates. Plans can no longer retroactively deny previously approved inpatient admissions except for fraud or obvious error. These rules improve transparency and response times but do not eliminate the administrative burden agencies face in submitting, tracking, and appealing authorizations.
Why are Medicare Advantage denial rates higher than Traditional Medicare?
A 2022 HHS Office of Inspector General report found that 13% of prior authorization requests denied by MA plans would have been approved under Traditional Medicare coverage rules, and 18% of payment requests denied by MA plans met standard Medicare coverage and billing rules. MA plans use utilization management criteria that are often stricter than CMS requirements, and they have financial incentives to control service utilization. Prior authorization denials in MA jumped 56% in recent years. The burden of proving a denial was incorrect falls on the home health agency, requiring documentation that clearly establishes medical necessity, skilled need, and homebound status to the plan's satisfaction.
How does Medicare Advantage affect home health agency revenue?
MA affects agency revenue through three mechanisms simultaneously. First, reimbursement rates are often 15% to 30% lower than Traditional Medicare for the same patient profile. Second, the administrative cost per patient is higher because of prior authorization, concurrent review, and appeals requirements. Third, payment timelines extend to 45 to 90 days compared to 14 to 30 days under Traditional Medicare, creating cash flow pressure. Combined with CMS finalizing a 1.3% aggregate reduction in Traditional Medicare home health payments for CY 2026, agencies face margin compression from both sides of their payer mix.
Should home health agencies accept every Medicare Advantage plan?
Not necessarily. Agencies should analyze each MA contract on a per-episode basis, including the reimbursement rate, average days to payment, denial rate, and appeal success rate. Some MA plans pay rates comparable to Traditional Medicare and process claims efficiently. Others pay significantly below cost, deny at high rates, and take months to pay. The agencies managing the MA transition most effectively have made deliberate decisions about which contracts are operationally and financially sustainable, and have exited or renegotiated contracts that consistently lose money on a fully loaded cost basis.
How can automation help agencies manage Medicare Advantage patients?
Automation addresses the three highest-cost operational areas of MA management. Prior authorization tracking systems connected to the EMR ensure authorizations are submitted, monitored, and renewed before they expire. Pre-visit automation extracts referral data and pre-populates clinical documentation so that authorization requests include complete clinical pictures from the start, reducing denial rates. And automated eligibility verification catches payer issues before the start of care visit rather than after the claim is denied. Copper Digital's AI agents handle referral extraction, eligibility verification, and EMR pre-population in approximately 3 minutes per referral, which is particularly valuable for MA patients where documentation completeness directly determines whether the authorization is approved.
If your MA payer mix is growing and your margins are shrinking, request a free operational assessment at copperdigital.com/contact-us. We will map your current intake-to-payment cycle, identify where MA-specific friction is costing you time and revenue, and show you what changes in 90 days.
TL;DR
More than half of Medicare beneficiaries are now enrolled in Medicare Advantage plans, and that number is still climbing. For home health agencies, this shift means lower reimbursement per episode, longer payment cycles, more prior authorization requirements, higher denial rates, and a fundamentally different operational model than Traditional Medicare. Prior authorization denials jumped 56% in recent years, and a 2022 HHS OIG report found that 13% of denied MA prior authorization requests would have been approved under Traditional Medicare. The new CMS Interoperability and Prior Authorization rule, effective January 2026, requires MA plans to respond to urgent requests within 72 hours and standard requests within 7 calendar days, but agencies still carry the operational burden of submitting, tracking, and appealing. This blog breaks down what Medicare Advantage actually changes for home health operations, where agencies are losing money, and what operational infrastructure you need to survive an MA-dominant payer mix.

