Blog
Apr 27, 2026
The Problem with Healthcare AI is that Most of it doesn't Work

By Nathan Hayman | CEO, Rivvi.ai

I like to start every conversation with this: we were building AI in healthcare when AI wasn't cool.
Two years ago, voice AI in healthcare was taboo. Not skeptical. Not early. Taboo. If you told someone you were having an AI system make phone calls to patients, they looked at you like you were describing something illegal. People wanted governance documentation, safety frameworks, and clinical oversight structures before they would even consider letting you run a pilot. That was before most people had heard of large language models, let alone used them.
We built anyway. We had no choice, honestly. The problem was right in front of us, the solution was obvious, and waiting for the industry to become comfortable with AI was not a strategy.
Two years later, we are bootstrapped profitable. We have gone from 2,000 outbound calls a month to over 60,000. We work with the largest independent medical group in the Southeast, community pharmacy chains, clinical trial organizations, and the New York City Department of Health. Every single deal we have closed came from a LinkedIn DM. We have not raised a VC round, and I think that turned out to be exactly right.
Here is what building this company actually taught me.
How It All Started
I am not going to dress up the origin story. I was not analyzing market opportunity or studying TAM. My girlfriend was coming home every single day from her job at a primary care call center, and she was miserable.
She was one of thirty call center agents who were handed a giant Excel spreadsheet and told to call patients for whatever campaign was running that week. Nobody wants to receive those calls. Nobody wants to make them. The agents were spending less than five percent of their time on actual outbound work because the process was so painful and inefficient. The notes column in the spreadsheet was the only record of what happened on any call. Patient said this, retry tomorrow. That was the intelligence pipeline.
From a technical standpoint, this was a blueprint for automation. You have structured data coming in. You need outbound calls to go out. You need structured insights to come back. This is not a complicated workflow. The fact that thirty human beings were doing it manually with an Excel sheet was not a healthcare problem. It was a process problem with an obvious fix.
The first goal, genuinely, was to stop my girlfriend from crying. We accomplished that pretty early. I like to say I am the best boyfriend ever because I changed her job. The reality is we changed the jobs of thirty call center agents. They do not do outbound anymore. We took them from 2,000 outbound calls a month to 60,000. They man inbound now, and their inbound handle rate actually went up.
I never say we are building AI products. I never say we have the best AI. We are solving a problem. If voice AI needs to be part of the solution to actually solve it, that is what it needs to be. But we are solving the problem. |
Coming From Outside Healthcare Is an Advantage
I dropped out of college. I taught myself to engineer. I worked the 4 AM shift at Target, moving boxes while doing online engineering education, and eventually told my manager I quit because I got a software job. I have built products for solar companies, CBD supplement brands, and e-commerce. I worked in Las Vegas, building and developing solutions for seventeen different portfolio companies simultaneously, working from the moment I woke up until the moment I fell asleep.
None of that background is what you would put on a healthcare AI founder's resume.
But here is the thing about coming into healthcare from outside: you are genuinely shocked by what you see. Everyone who has been in the industry for years has normalized the dysfunction. The Excel sheets, the manual processes, the fax machines, and the complete absence of what would be considered basic technical infrastructure in any other industry. When you come from outside, and you see a large primary care organization running its outreach program on a spreadsheet in 2023, you are not desensitized to it. You are standing there thinking: This cannot be real.
That shock is actually useful. It prevents you from accepting the standard explanation, which is that healthcare is just complicated and slow, and that is how it works. Healthcare is complicated. But Excel sheets are not a compliance requirement. Manual outbound calling is not mandated by regulation. These are just bad processes that nobody has replaced because the people inside the system have stopped seeing them as replaceable.
The best thing I did early on was talk to everyone. Call center agents. Their managers. Population health teams. Every role is involved in the workflow. Not to validate my solution, but to understand the actual problem at every layer. By the time we built anything, we understood the workflow better than most people who had been working in it for years.
The EMR Problem Is Not What You Think It Is
Here is the thing that blew my mind and that I think every healthcare technology builder needs to understand before they get into this space.
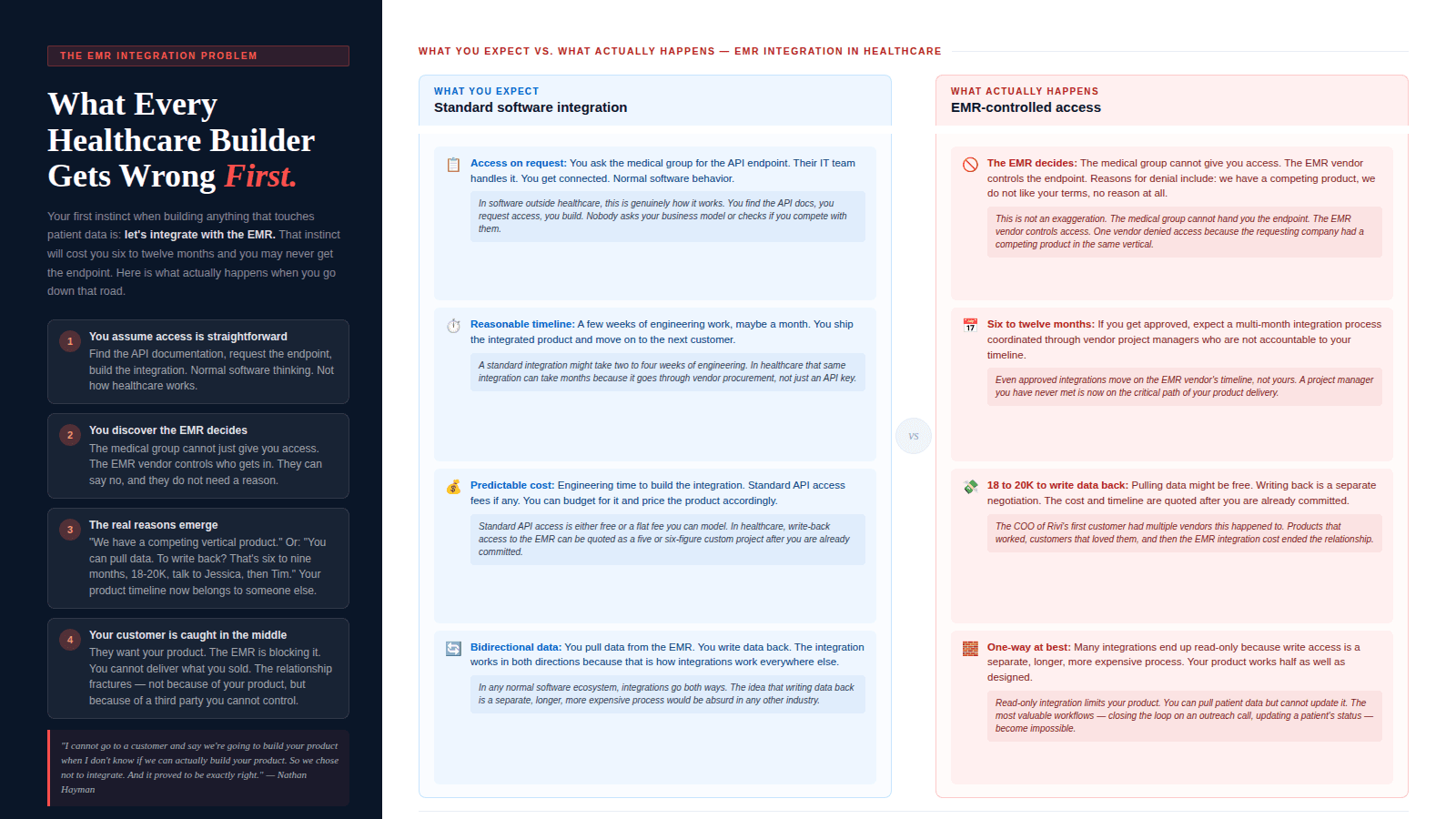
If you come from outside healthcare and you think about building anything that touches patient data or clinical workflows, your first instinct is: we need to integrate with the EMR. Scheduling an appointment? API call. Confirming a visit? API call. Pulling patient data? API call. This is normal software thinking. You find the documentation, you figure out the integration, you build it.
That is not how it works in healthcare.
When I spoke with the COO of our first customer, which was a large enterprise medical group with its EMR vendor as an investor in the company, I learned something that fundamentally changed how we build. The COO told me about multiple vendors they had worked with. Products that worked. Customers who loved them. And then the time came to integrate with the EMR, and everything fell apart.
The EMR vendor does not have to give you access. The medical group cannot just hand you an endpoint. The vendor decides whether you get access, on what timeline, at what cost. And the reasons they say no are not always clinical or regulatory. One vendor was told no because the EMR had a competing product in the same vertical. Another was told yes for data pull, but then informed that writing data back would take six to nine months, cost up to twenty thousand dollars, and required coordination with a project manager and a timeline that had nothing to do with the product they were trying to build.
In any other software industry, competing tools integrate with each other freely because they are competing on features in an open market. That competition drives better products for users. In healthcare, the EMR decides who gets access to the core infrastructure. When the gatekeepers can say no with no explanation required, innovation stalls. That is not a technology problem. It is a structural one.
We made the decision not to integrate with the EMR. Early on, that felt risky. My co-founder thought we would have no customers without it. But the reality was that we could deliver value without it, and the moment you tell a potential customer you integrate with the EMR, you are triggering a twelve-month procurement and integration process that has nothing to do with whether your product works. We did not want to promise something we could not control.
That decision turned out to be exactly right.
If you tell a customer you integrate with the EMR, you are triggering a process that might take twelve months and has nothing to do with whether your product actually works. We choose not to. If we can deliver value without it, why would we add a dependency we cannot control? |
The LinkedIn Post That Changed Everything
We spent about six or seven months building in stealth. No public presence, no announcements, no product pitches. Just building.
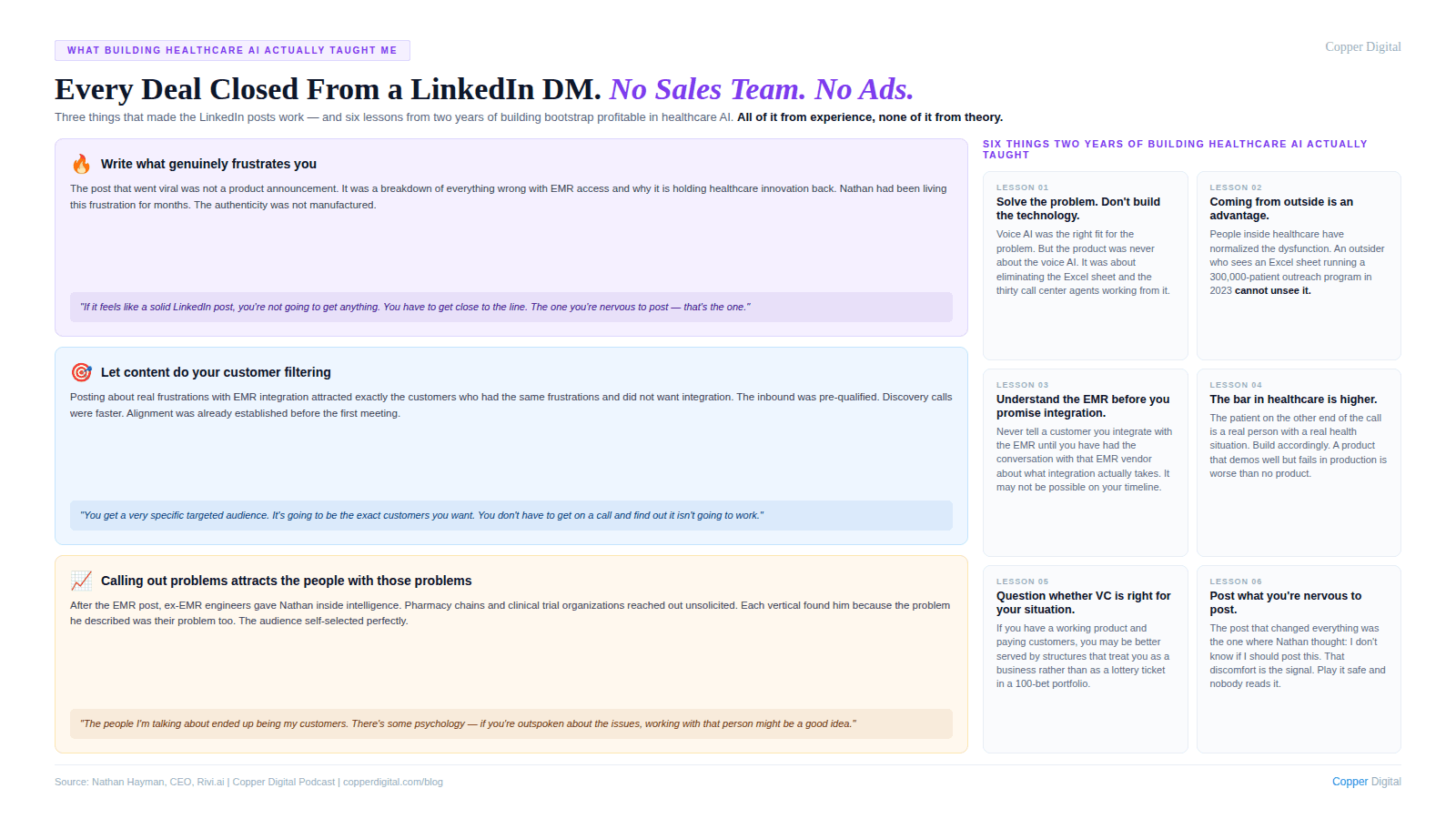
When I decided to post on LinkedIn for the first time, I did not think about the algorithm or the optimal posting time or what format would maximize engagement. I thought about what I was genuinely frustrated about and what I could talk about for hours without running out of things to say. The EMR situation was the obvious answer.
I was nervous about posting it. When you go out publicly and talk about something that is clearly going to get a reaction, there is a moment before you hit post where you think: is this the right call? I did some research before I posted and found that Marc Benioff at Salesforce had done something similar in the early days, publicly calling out the incumbent software players, and those players ended up becoming his customers. That gave me enough confidence to go ahead.
The post went what I can only describe as viral for healthcare LinkedIn. My DMs were full within hours. Not just people complaining about EMRs. Ex-EMR engineers giving me insight into why things work the way they do. People from verticals I had not thought about saying: we have the same problem, does your solution work here? A community pharmacy chain reached out and said: we have a giant Excel sheet of patients we need to call, is this something you could help with?
Every deal we have closed since then came from a LinkedIn DM. No paid marketing. No sales team. No outbound prospecting. Just posts that were honest about real problems, real frustrations, and real things I knew from experience.
The filter this creates is actually valuable beyond the distribution. When you are publicly specific about the problems you are solving and the way you think about them, the people who reach out to you are the exact customers you want. They are not asking whether you integrate with the EMR. They already know you do not and they agree with your reasoning. The discovery process becomes almost frictionless because the alignment is already established before the first call.
My advice to anyone trying to get traction through content: write about something you have actually experienced. Write about something that, right before you post it, makes you think maybe I should not post this. That is the post that will land. If it feels like a solid LinkedIn post, you are playing it too safe.
Why Bootstrap Worked for Us
We were not ideologically opposed to raising money. We applied to YC multiple times. We had conversations with Andreessen Horowitz after they included us in their B2B voice agent market map. None of it materialized, and I genuinely believe that was the right outcome.
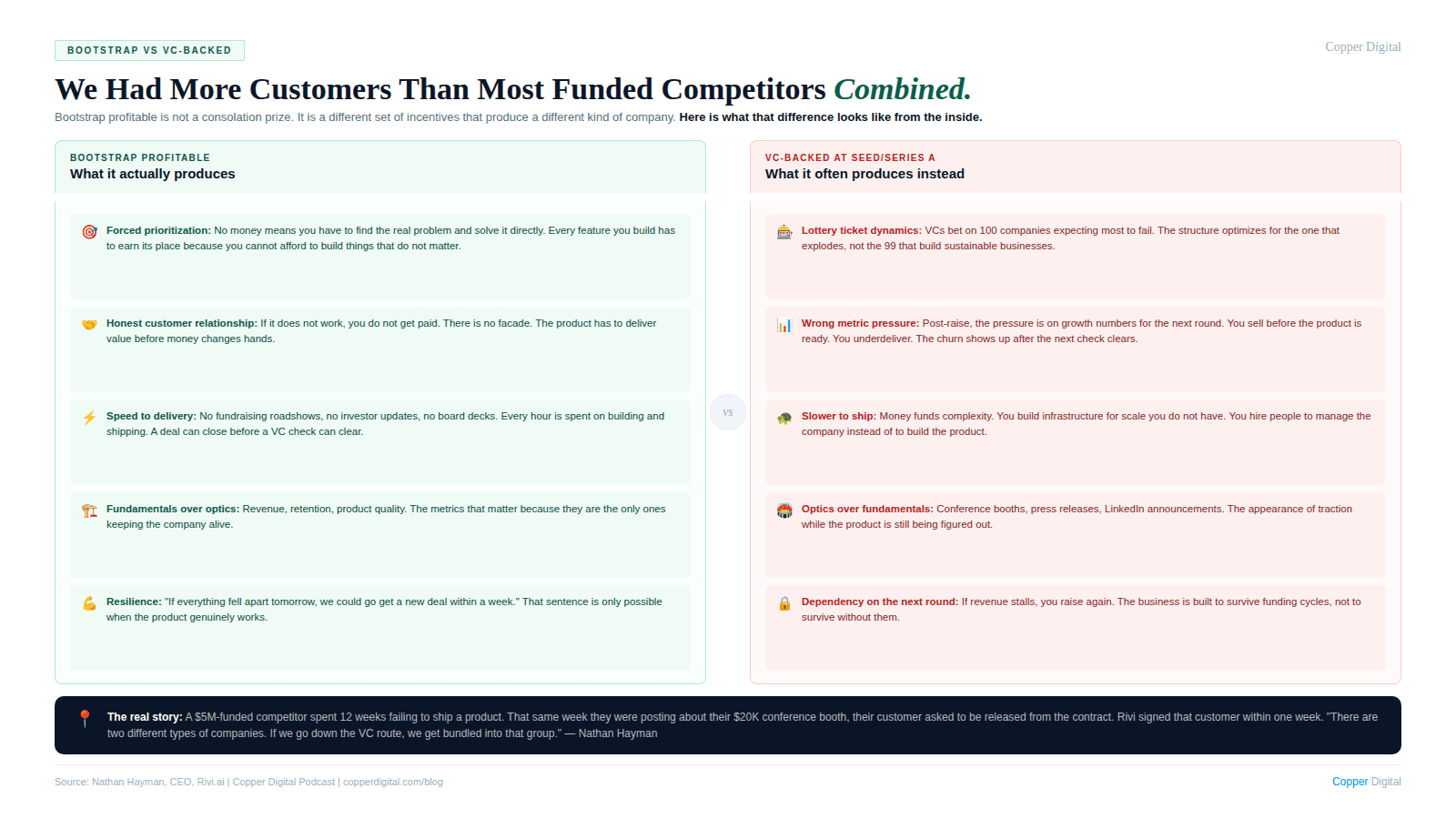
Here is my honest read on VC for a company like ours. If you are a pre-seed company with an idea and no customers, VC is the right vehicle. But if you have a working product, paying customers, and real business fundamentals, the VC model is designed to treat you as a lottery ticket. They are betting on a hundred companies hoping one returns the fund. That math requires most bets to fail. I do not want to be optimized for that.
What changed my thinking was a conversation about growth equity, which is a different structure that bets on companies with fundamentals rather than on ideas with potential. The distinction matters because it changes what you are optimizing for.
The more I watched VC-backed healthcare AI companies, the more clear the contrast became. We had more customers than most of them combined. We were doing more call volume than most of them combined. Some of them were series A companies that were still in what I would describe as the idea phase. We do not have a facade behind what we are doing. We have a product that works and customers who pay for it. If everything fell apart tomorrow, we could go get a new deal within a week. That is not something a company that has raised its way to scale can usually say.
Too much capital is its own problem. When money is not a constraint, prioritization becomes difficult. You start solving problems that are not the most important ones. You build infrastructure for scale you do not have yet. You hire people to manage the complexity of the company rather than to build the product. The constraint of bootstrap forces you to find the real problems and solve them in the most direct way possible.
What Voice AI in Healthcare Actually Requires
People ask me constantly about the technology choices we made and what makes voice AI actually work in healthcare as opposed to just in demos.
The honest answer is that the clinical part of the problem is simpler than most people think. The hard part is everything around it.
Getting an AI to have a reasonable phone conversation with a patient about an appointment reminder or a medication refill or a care gap campaign is not technically difficult in 2025. The frontier models are capable of handling that. What is difficult is building the full infrastructure around that conversation: how does the data get in, how does the AI handle edge cases and escalations, how does the output get structured and stored, how does the whole thing operate reliably at scale across tens of thousands of calls a month.
The governance question is real. When we started, we had to explain what AI was before we could explain what we were doing with it. Now people ask for HIPAA compliance documentation, security architecture reviews, BAA provisions, and clinical oversight frameworks. That is appropriate and we have all of it. But the companies that treat governance as a checkbox exercise are going to run into problems. The patients on the other end of these calls are real people with real health situations. The bar for what counts as working correctly is higher in healthcare than in pizza delivery.
The other thing I will say is that the specific use case matters more than the technology. The same conversational AI infrastructure that works for appointment reminders works for medication adherence outreach works for clinical trial enrollment screening works for pharmacy refill campaigns. The underlying capability is consistent. What changes is the workflow integration, the script logic, the data flows, and the escalation protocols. Those are deeply specific to each use case and each customer. The companies that try to build one generic solution and apply it everywhere are going to find that the edges are where healthcare problems live.
The Difference Between a Product That Works and a Product That Ships
Three weeks before I wrote this, we were introduced to a company that kept asking the same question on our first call: how fast can you get this live?
I found the question a little unusual. That is usually not the biggest priority for healthcare organizations. I said a week, which was conservative. I wanted to under-promise. In the back of my head I was thinking a day, but I said a week.
Turns out they had been working with another voice AI company for twelve weeks. This company had raised five million dollars in a seed round the year before. Twelve weeks later, nothing had been delivered. The customer asked to be released from the contract on a Friday. We signed them the following week.
That same voice AI company was posting about their twenty-thousand-dollar conference booth on social media the same week they were releasing that customer from their contract.
This is the reality of a lot of healthcare AI right now. VC-backed companies that are optimized for fundraising metrics rather than product delivery. The money creates a performance pressure that is oriented toward the wrong things. You raise a round, you need to show growth, you sell before the product is ready, you underdeliver, and the customer churns. The money funds the next round before the churn shows up in the numbers.
We do not have that problem because we do not have that structure. If we do not deliver value, we do not get paid. That is a much simpler and more honest relationship with our customers.
What I Would Tell Someone Starting Now
If you are thinking about building in healthcare AI, here is what I would actually tell you.
Find the problem before you find the technology. The problem we are solving was a giant Excel sheet and thirty call center agents. Voice AI was the right tool for it. But the product was never about the technology. It was about eliminating that workflow.
Get close to the actual work. Talk to the call center agents. Talk to the clinical pharmacists who are spending forty hours a week on the phone. Talk to the people doing the job that needs to change. They will tell you everything you need to know.
Understand the EMR situation before you promise integration. Do not tell a customer you will integrate with their EMR until you have personally had the conversation with that EMR vendor about what integration actually takes.
Post what you are actually frustrated about. Not what you think the algorithm wants. Not a polished company announcement. The thing you are nervous to post because it might burn a bridge. That is the one that will resonate.
Question whether VC is the right vehicle for your specific situation. If you have a working product and paying customers, you may be better served by structures that treat you as a business rather than as a lottery ticket.
The bar for healthcare is higher. The patient on the other end of the call is a real person with a real health situation. Build accordingly.
Rivvi.ai handles conversational AI and voice-based patient outreach for healthcare organizations across primary care, pharmacy, clinical trials, and more. If you have a workflow that involves calling patients, reach Nathan directly at Rivvi.ai or find him on LinkedIn. |
TL;DR
Nathan Hayman is the CEO of Rivi.ai, a conversational AI company handling voice-based patient outreach for primary care groups, pharmacies, and clinical trial organizations. He built it two years ago when AI in healthcare was genuinely taboo, without raising a VC round, and without integrating with a single EMR. Every deal he has closed came from a LinkedIn DM. In this post, Nathan shares the origin story behind Rivi, why he made the controversial call to skip EMR integration, what his viral LinkedIn post actually said and why it worked, and what two years of building a bootstrap profitable healthcare AI actually taught him about solving real problems versus shipping impressive demos.
About the Author
Nathan Hayman is the founder and CEO of Rivvi.ai. He is a self-taught engineer and college dropout who built his first software product while working the 4 AM shift at Target. Before founding Rivvi, he built digital products across seventeen different industries. He started Rivvi.ai two years ago when AI in healthcare was genuinely taboo, and has grown it to a bootstrap profitable company handling over 60,000 patient calls per month. He is featured in the Andreessen Horowitz B2B voice agent market map.

