Blog
Jan 3, 2026
Why Section GG Errors Are Your Biggest Revenue Risk

Arvind Sarin

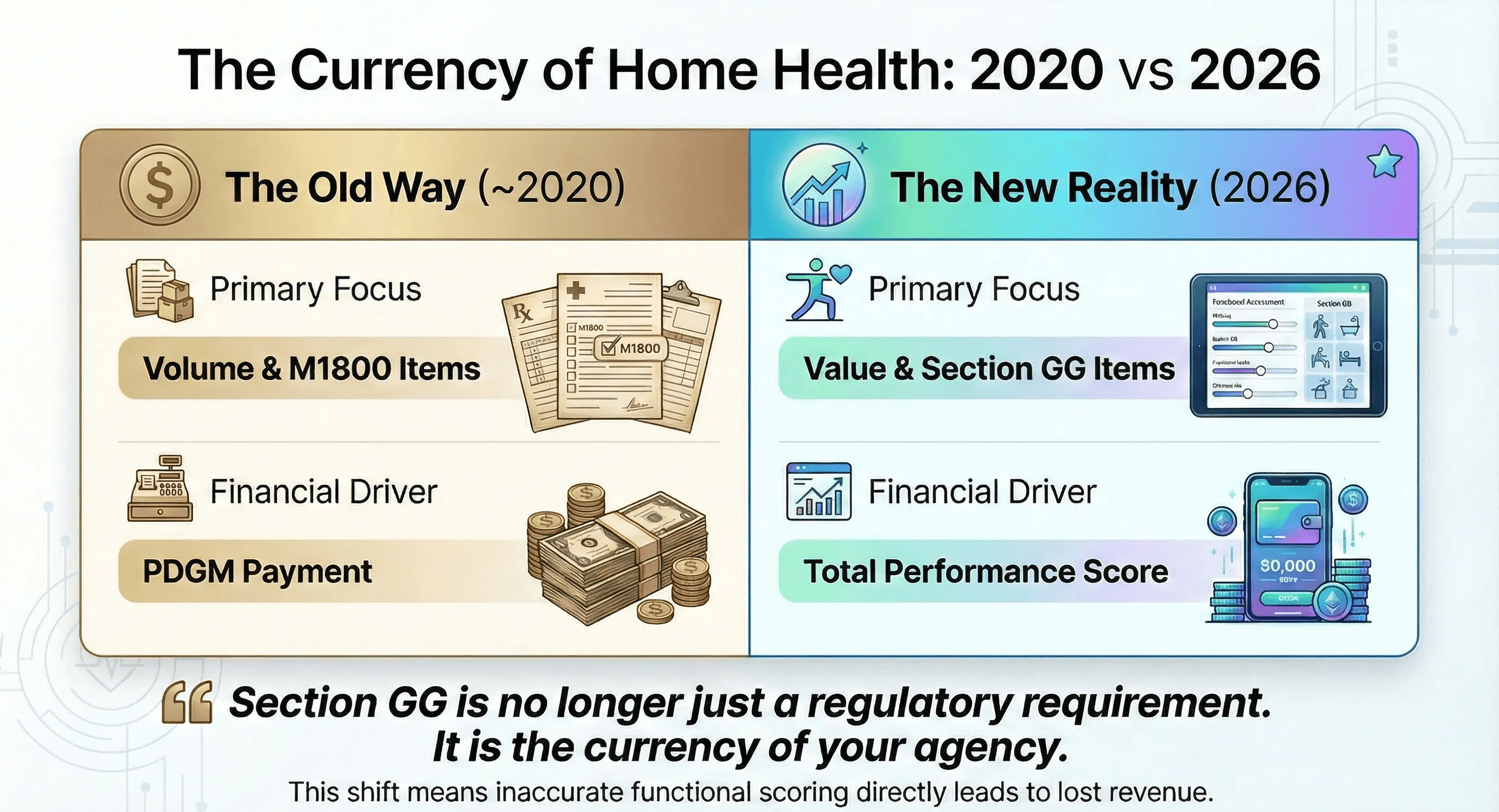
If you are a Home Health Director of Nursing in 2026, you know that Section GG is no longer just a regulatory requirement. It is the currency of your agency.
For years, we treated Section GG as a secondary dataset. We focused heavily on the M1800 items because that was where the money was. But under the fully matured Home Health Value-Based Purchasing (HHVBP) model, the script has flipped. Section GG Functional Abilities now drives a massive portion of your Total Performance Score.
This shift has exposed a dangerous weakness in many agencies. While your clinicians are experts at wound care and medication management, they are often struggling with the rigid non-clinical logic of functional scoring.
The result is "Revenue Leakage." Every time a nurse marks a patient as "Independent" when they actually require "Supervision," you are essentially writing a check back to CMS. You are telling the government that your patient is perfect, and therefore, you do not deserve to be paid for improving them.
We need to dive deep into the specific, highly technical errors that are happening in living rooms across the country right now.
Subjectivity vs Definitions
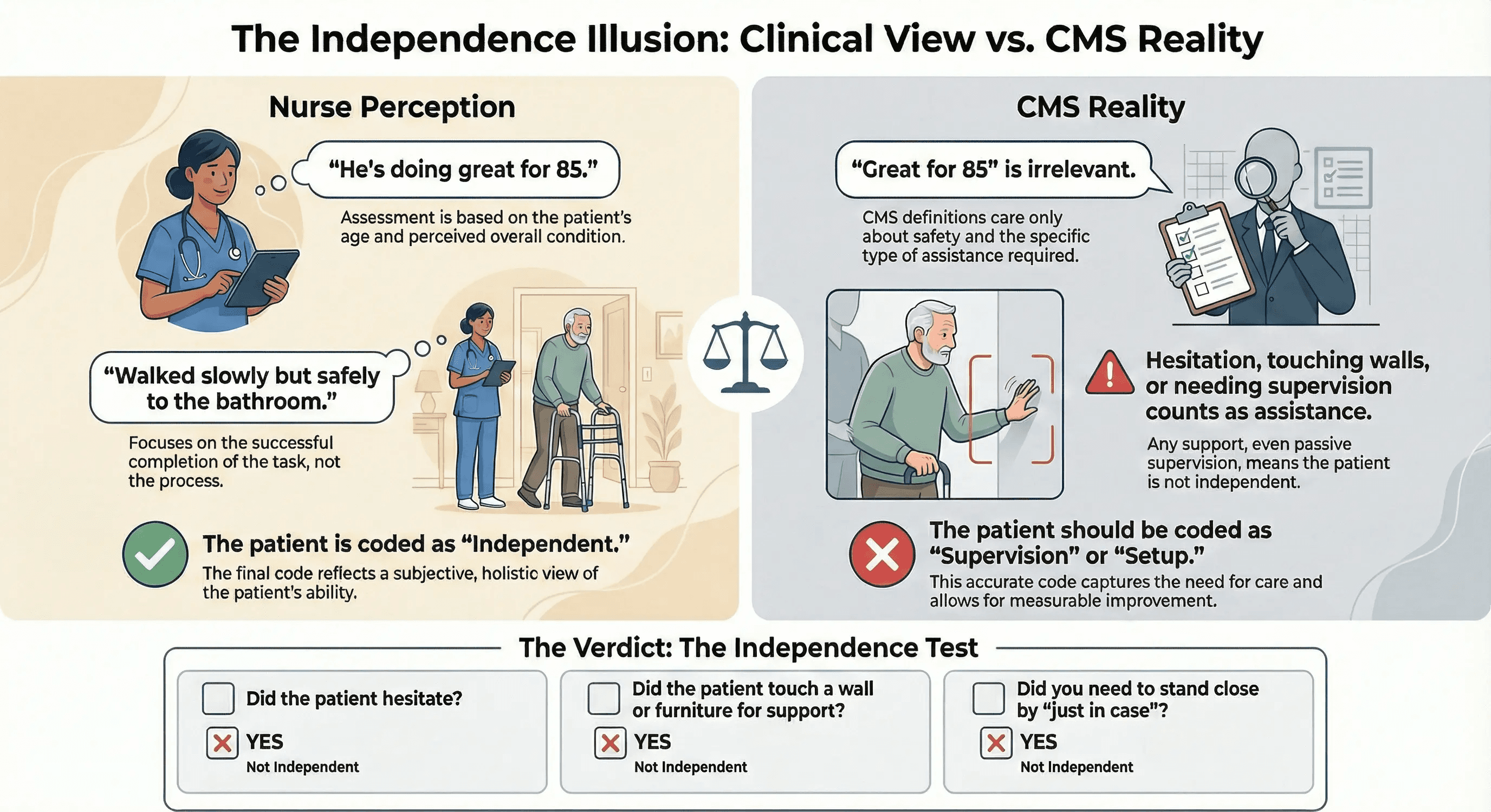
The root cause of most Section GG coding errors is the difference between "Clinical Judgment" and "CMS Definitions."
Clinically, a nurse sees a patient walk to the bathroom slowly but safely. She thinks that he is doing great for 85. She marks him as Independent.
But the CMS OASIS Manual does not care about "great for 85." It cares about safety and assistance.
Did the patient hesitate? Did they touch the wall? Did the nurse have to stand close by just in case?
If the answer to any of those is yes, then that patient is not Independent. They are at least "Setup/Clean-up Assistance" (Code 05) or "Supervision/Touching Assistance" (Code 04).
By missing this nuance, your agency loses the opportunity to show improvement. When that patient actually becomes independent at discharge, you get zero credit because you claimed they started at the finish line.
Error 1: The Ambulation vs Transferring Confusion
One of the most frequent areas of failure is the distinction between transferring and ambulating.
In the real world, these activities blur together. You stand up (transfer), and then you walk (ambulate). But in the OASIS-E logic, these are distinct mathematical events that must be scored separately.
The Scenario
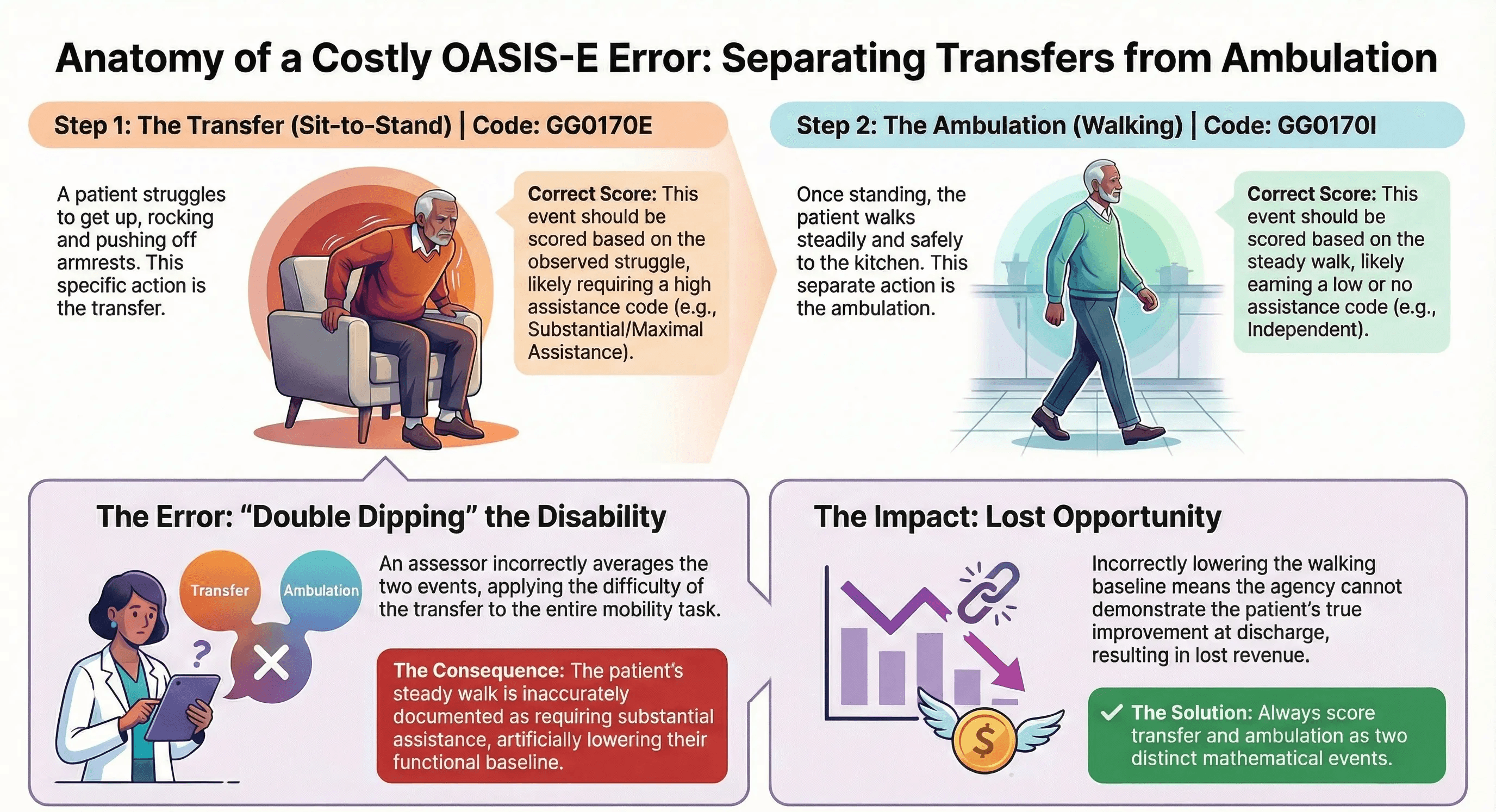
A patient is sitting in a recliner. The nurse asks them to walk to the kitchen. The patient struggles to get up, rocking back and forth three times before finally pushing off the armrests to stand. Once standing, they walk steadily to the kitchen.
The Coding Error
The nurse sees the struggle. She codes GG0170 (Mobility) as "Substantial/Maximal Assistance" because the patient had such a hard time.
The Correction
This is a coding failure. The struggle to stand up belongs to GG0170E (Chair/Bed-to-Chair Transfer). The walk to the kitchen belongs to GG0170I (Walk 10 feet).
If the patient walked steadily once they were up, then the Ambulation score should likely be better than the Transfer score. By conflating the two, the nurse effectively "double dips" the disability, which lowers the baseline for walking artificially. Or worse, she averages them and ignores the specific deficit in the transfer that needs therapy.
Error 2: The Helper Trap
This is the single most expensive error in home health documentation.
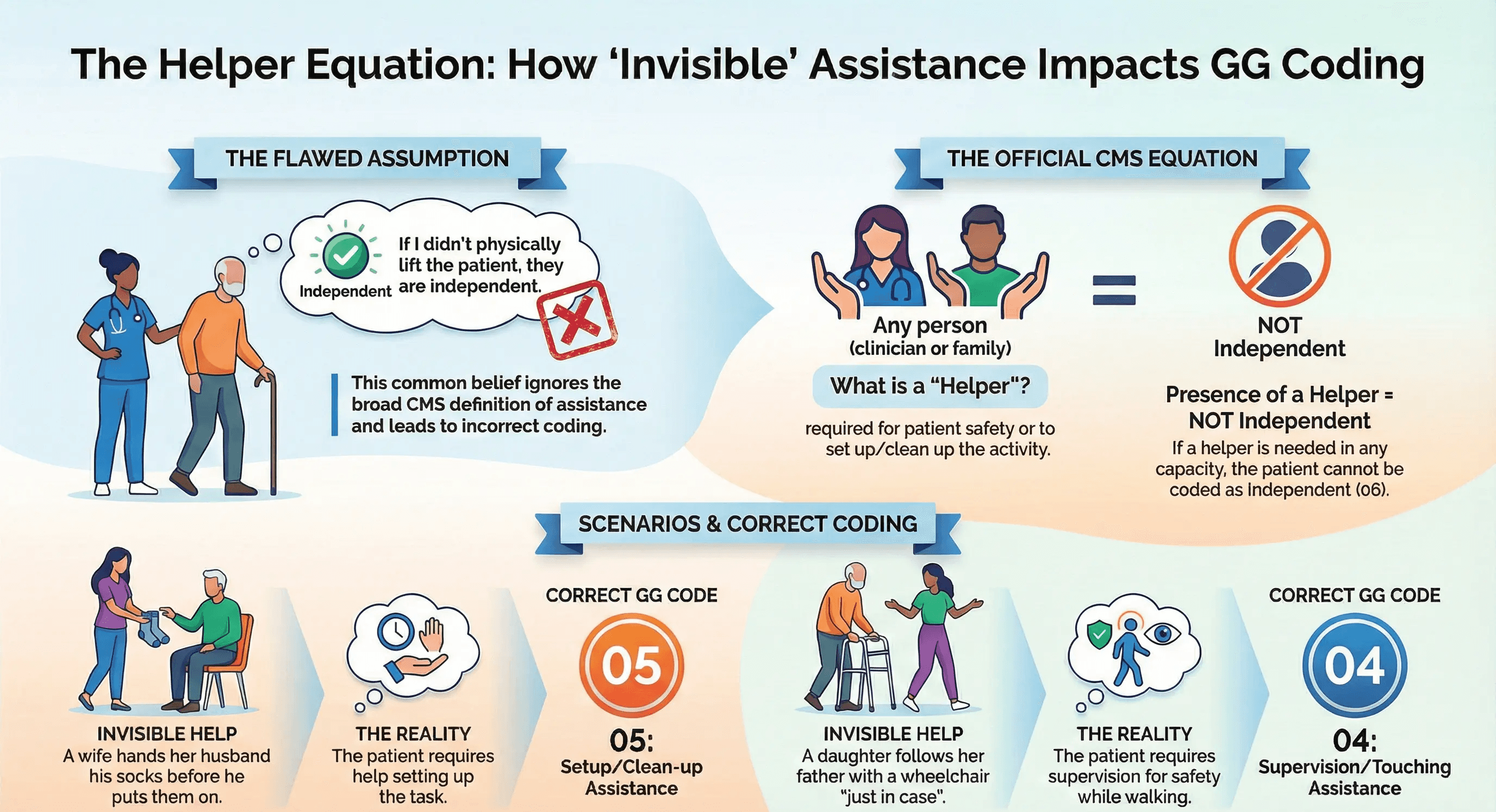
The definition of Code 01 (Dependent) or Code 02 (Substantial/Maximal Assistance) relies entirely on the concept of a "Helper."
Many nurses believe that if they didn't physically lift the patient, then they didn't provide assistance. They simply watch the patient struggle and then document "Independent."
The CMS Rule: If a helper (the nurse or a family member) is present and required for safety, that counts as assistance.
If a patient cannot put on their socks without their wife handing them to them, they are not Independent. He requires "Setup/Clean-up Assistance" (Code 05).
If a patient can walk alone but his daughter follows him with a wheelchair "just in case," he is not Independent. He requires "Supervision" (Code 04).
These small distinctions are worth thousands of dollars in reimbursement. They define the "Improvement Gap." If you miss the helper, you close the gap.
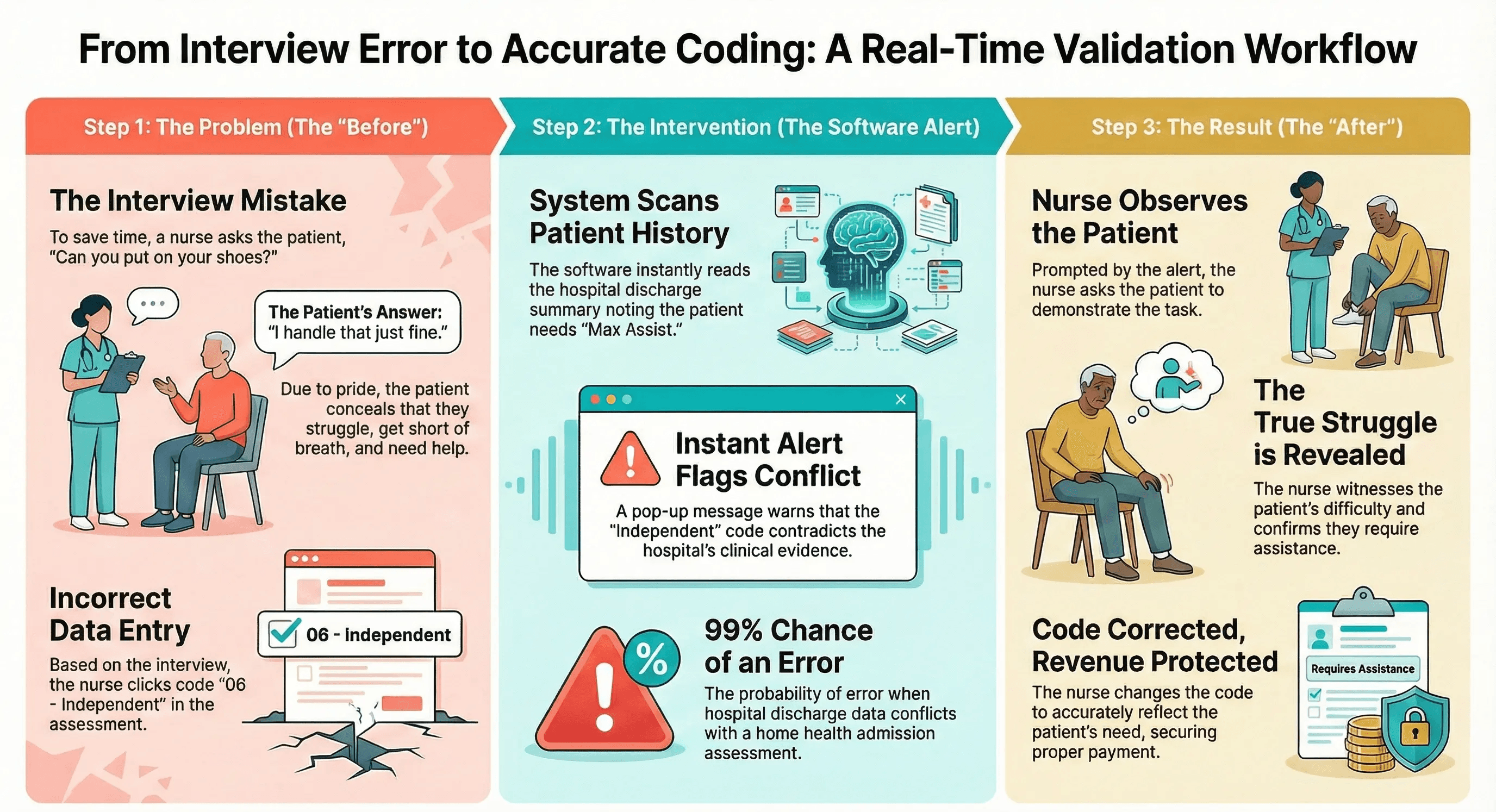
Error 3: The Interview Mistake
Why do these errors happen? Usually, it comes down to time.
Nurses are busy. Instead of asking the patient to demonstrate putting on their shoes, they ask the patient, "Can you put on your shoes?"
Patients lie. They don't do it maliciously. They do it out of pride. No 80-year-old man wants to admit to a stranger that he can't dress himself.
The Patient Says, "Oh yes, I handle that just fine." The Reality: It takes him 20 minutes, he gets short of breath, and his wife usually finishes tying the laces.
If the nurse codes based on the interview, she codes Independent (06). If she codes based on observation, she codes Partial/Moderate Assistance (03).
That difference is the difference between a profitable episode of care and a break-even one.
The Solution Is Deterministic Validation
You cannot fix this problem with more training. You have likely already done five in-services on OASIS-E this year. The rules are too complex, and the nurses are too tired to memorize every page of the manual.
You need a safety net that catches the error before the claim is submitted.
This is where Deterministic Validation comes in.
At Copper Digital, we do not rely on "AI guessing." We rely on "AI proving."
Our system reads the entire clinical history. It sees the Physical Therapy notes from the hospital, which state "Patient requires Max Assist for lower body dressing."
When your nurse attempts to click "Independent" for GG0130E, our system instantly flags the discrepancy.
Alert Hospital PT noted Max Assist 3 days ago. Patient interview contradicts clinical history. Please verify via observation.
This is not the software telling the nurse she is wrong. It is the software asking her to be sure.
Nine times out of ten, the nurse stops. She realizes she didn't actually watch the patient dress. She goes back. She asks the patient to try. She sees the struggle. She corrects the code.
Protecting Your Margins
In 2026, accuracy is not just about compliance. It is about survival.
You are providing excellent care. Your therapists are working miracles, getting patients from bedbound to walking. But if your admission data fails to capture the starting point, you will never get credit for that finish line.
Don't let Section GG coding errors rob you of the revenue you have earned. Equip your team with the tools that make precision the default, not the exception.
See Copper Digital in action. Let us show you how Deterministic Validation can secure your VBP score today.
Frequently Asked Questions
Why is Section GG more important than M1800 items now
Under the 2026 HHVBP model, CMS re-weighted the scoring system. While M1800 items still impact your PDGM payment, Section GG items are heavily weighted in the "Functional Status" quality measure, which determines your annual payment adjustment (bonus or penalty).What is the difference between Code 05 and Code 06
Code 06 means "Independent," where the patient needs no help, no one is standing by, and no setup. Code 05 means "Setup/Clean-up Assistance," where the patient can do the task alone only after someone sets up the supplies or cleans up afterwards. This distinction is critical for capturing improvement.Can AI really catch these subjective errors
Yes, because they are rarely subjective when you look at the full dataset. If a hospital discharge summary says a patient cannot walk and the admission assessment says they are independent, there is a 99% chance of an error. AI detects that conflict instantly.Does this slow down the nurse's workflow
No, it actually speeds it up. By catching the error in real time, the nurse avoids the "Query Cycle" where QA managers have to reject the chart days later and ask for corrections. Getting it right the first time saves everyone time.Is it fraud to change the code after the AI alerts me
Not at all. The AI is simply presenting you with clinical evidence you may have missed. The nurse always makes the final decision based on their professional judgment and observation of the patient.

