Blog
Jan 14, 2026
Why Your Clinical Story Does Not Make Sense

Arvind Sarin
Imagine reading a novel where the main character is described as bedbound in Chapter 1. But then, in Chapter 3, that same character runs a marathon.
You would stop reading immediately. You would assume the author made a mistake or simply forgot what they wrote.
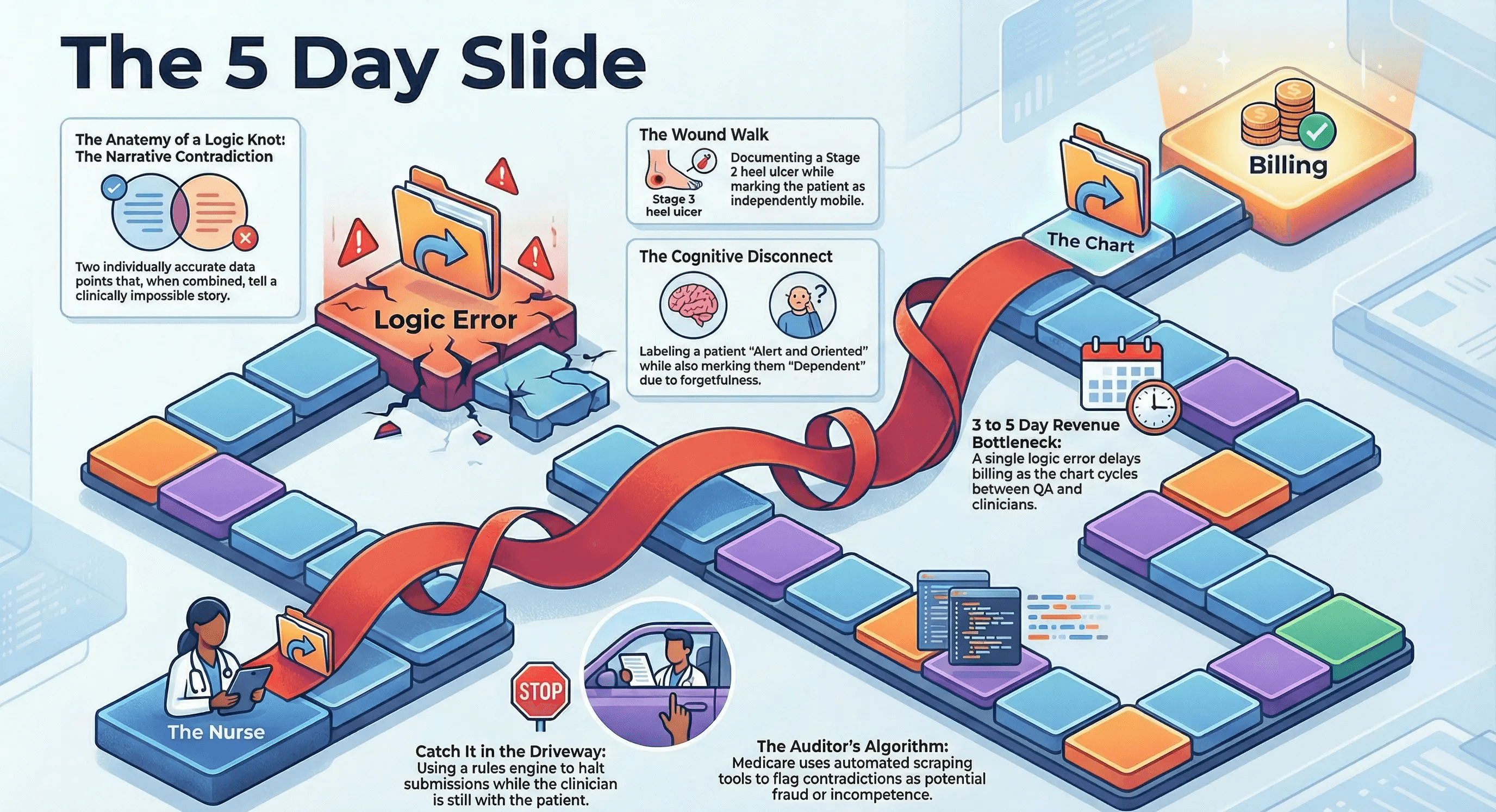
This exact scenario happens every day in home health charts. We call it "The Logic Knot."
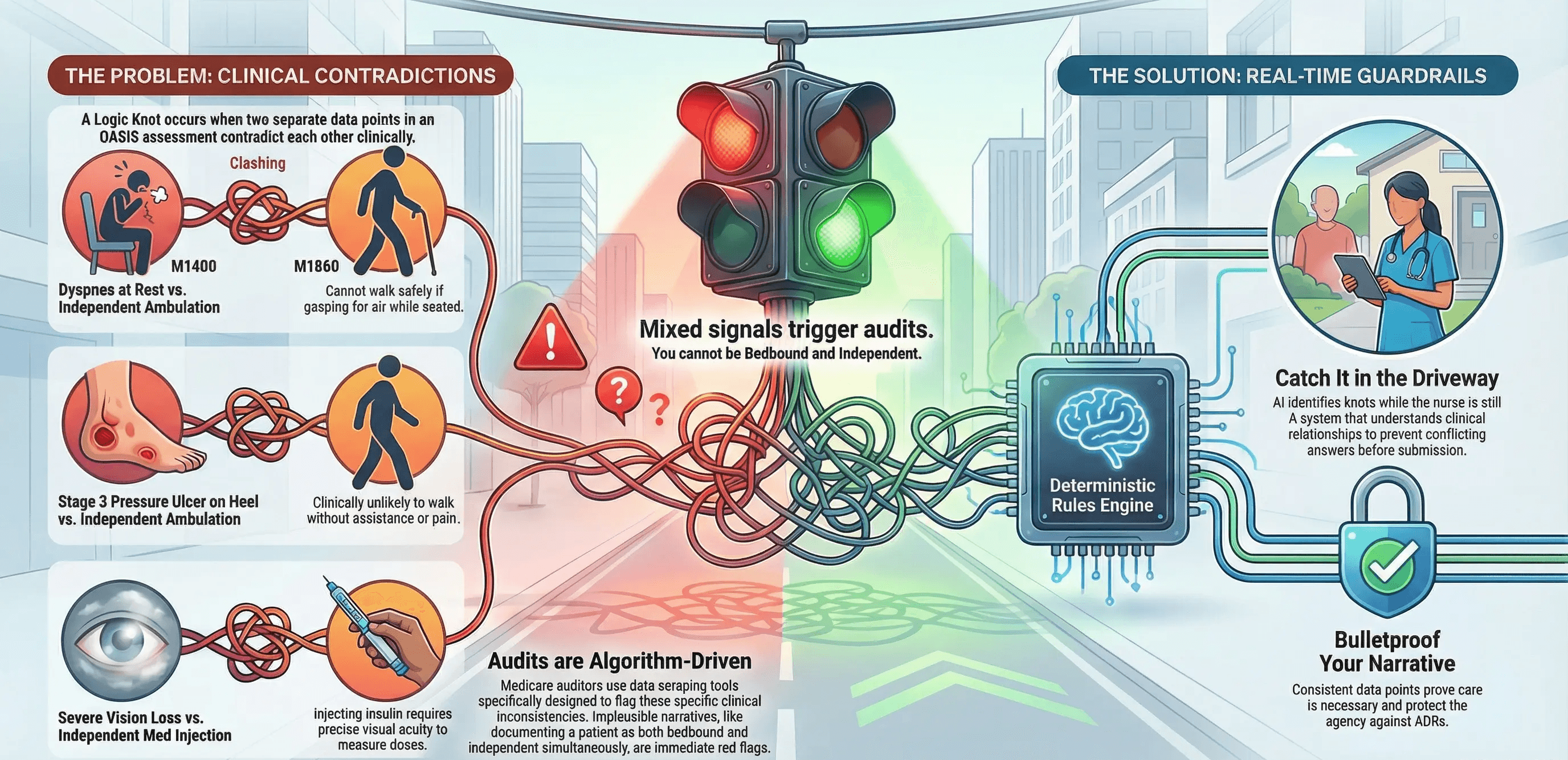
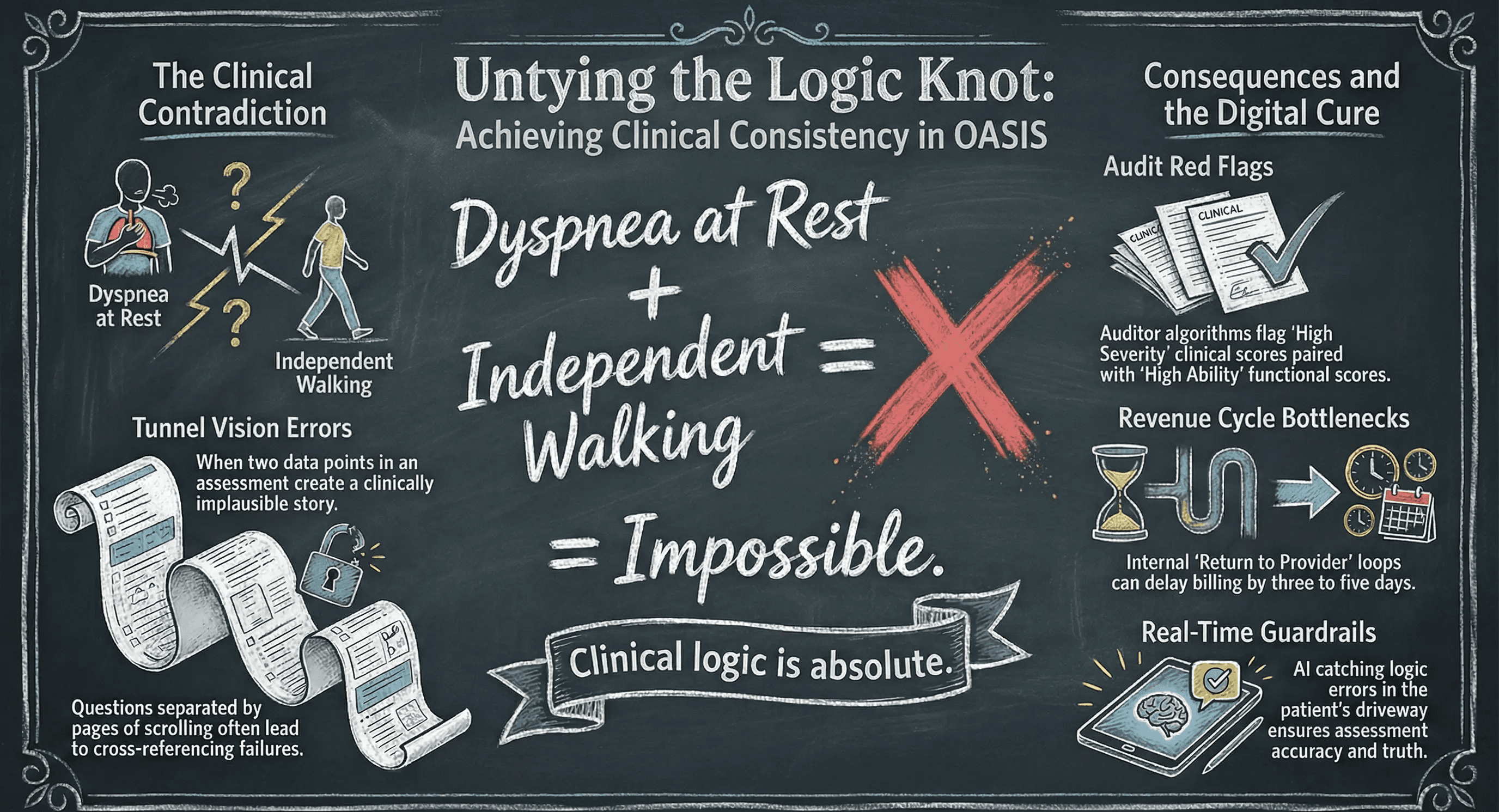
It occurs when two separate data points in an OASIS assessment contradict each other. Individually, they might look fine. But together they tell a clinically implausible story.
These knots are not just typos. They are the primary reason your charts get stuck in the QA queue. And they are the first thing a Medicare auditor looks for to deny a claim.
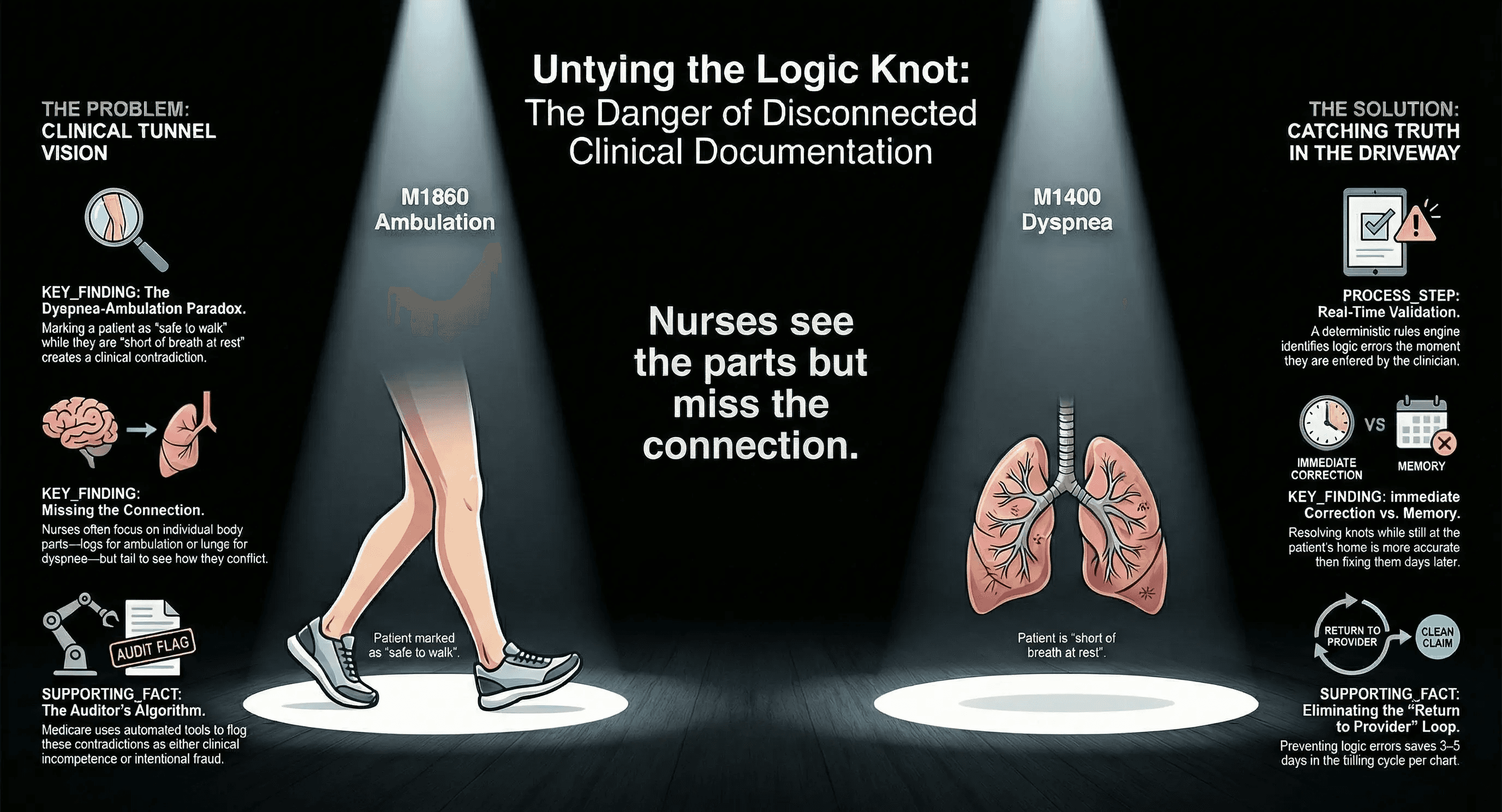
The Problem of Tunnel Vision
The OASIS assessment is a beast. With over 150 questions, it is impossible for a human brain to cross-reference every answer simultaneously.
The design of the form actually encourages these errors. Related questions are often separated by five or six pages of scrolling.
When a nurse answers M1860 (Ambulation), she is focusing entirely on the patient's legs. She watches the patient walk to the bathroom and grades them a "3" for safety.
Ten minutes and twenty screens later, she answers M1400 (Dyspnea). Now she is thinking about the patient's lungs. She notes that the patient is short of breath at rest.
Both answers might feel true in the moment. However, when you combine them, you have a Logic Knot.
How can a patient walk to the bathroom safely if they are gasping for air while sitting on the couch?
Three Common Logic Knots
The Dyspnea/Ambulation conflict is just one example. There are dozens of subtle contradictions that slip past even experienced nurses.
1. The Cognitive Disconnect The nurse marks the patient as "Alert and Oriented" in the Neuro section. But later in the IADL section, she marks them as "Dependent" for Medication Management due to "forgetfulness."
The Knot. If they are fully oriented, why do they forget their meds? Or if they forget their meds, are they truly fully oriented?
2. The Wound Walk The nurse documents a Stage 3 pressure ulcer on the patient's heel. Yet in the ADL section, she marks "Independent" for Ambulation.
The Knot. It is clinically unlikely that a patient with a severe open wound on their heel is walking without any assistive device or pain restrictions.
3. The Vision Trap The nurse notes the patient has "Severe Glaucoma" or significant vision loss. But later, she marks them as safe to "Inject Medication" independently.
The Knot Drawing up insulin requires precise visual acuity. If the patient cannot see well enough to read a newspaper, they likely cannot see well enough to measure a dose.
The Auditor's Algorithm
You might think these details are too small to notice. But Medicare auditors do not read charts with their eyes. They read them with algorithms.
They use data scraping tools specifically designed to find these Logic Knots.
If you submit a claim where the functional score says "High Ability" but the clinical score says "High Severity," the reviewer will flag it. They will assume you are gaming the system.
They interpret the contradiction in one of two ways.
Fraud: You are overstating the severity to increase the Case Mix Weight.
Incompetence You are overstating function to avoid a denial.
Either way, the result is an Additional Development Request (ADR). This halts your cash flow while you scramble to defend a chart that defends itself poorly.
The Cost to Internal Efficiency
Even if you escape the audit, the internal cost of Logic Knots is massive.
A Logic Knot cannot be fixed by a coder in the back office. A coder cannot decide if the patient is actually short of breath or actually safe to walk. Only the clinician knows the truth.
This triggers the dreaded "Return to Provider" loop. The chart goes from the nurse to QA. QA finds the knot. QA sends it back to the nurse. The nurse waits until the end of the day to fix it. The chart goes back to QA.
A single logic error can delay billing for three to five days. Multiply that by 50 charts a week, and you have a massive revenue cycle bottleneck.
The Deterministic Rules Engine
You cannot expect tired nurses to memorize the thousands of possible permutations of OASIS logic. They are focused on patient care, not data science.
You need a guardrail.
Copper Digital uses a "Deterministic Rules Engine" to prevent Logic Knots before they happen.
Unlike a standard spell checker, which looks for typos, our system looks for truth. It understands the clinical relationship between different questions.
The Guardrail in Action. If a nurse selects "Shortness of breath at rest" and then tries to select "Independent" for Ambulation, the system halts the submission.
It does not just say "Error." It poses the logic question directly to the nurse.
"You documented dyspnea at rest. Is the patient truly safe to ambulate independently, or do they require supervision due to respiratory distress?"
Catch It in the Driveway
The timing of this correction is critical.
If a QA manager catches a Logic Knot three days later, the nurse has to rely on memory. She is tired. She has seen 15 other patients since then. She might simply guess to make the error go away.
But if the AI catches the knot while the nurse is still in the patient's driveway, the truth is right in front of her. She can look at the patient again. She can clarify her assessment instantly.
This ensures that the chart tells a cohesive, consistent story from the first page to the last.
Protect Your Narrative
Your clinical documentation is a legal record. It needs to stand up to the Condition of Participation scrutiny.
When your data points align with your narrative, you bulletproof your agency against audits. You prove that your care is necessary and that your assessment is accurate.
Stop asking your QA team to untie these knots manually. Hand them a pair of scissors.
Untie your logic knots with Copper Digital.

