Blog
Jan 12, 2026
Why "Nice" Charting is Killing Your VBP Score

Arvind Sarin

Your field nurses are compassionate people. They entered this profession to heal and encourage. When they walk into a patient's home, they want to be a cheerleader. They want to tell Mrs. Jones that she is doing great and that her recovery is right on track.
That kindness is a clinical asset. But on the OASIS assessment, that same kindness is a financial liability.
We call this "The Nice Nurse Paradox."
It happens when a clinician subconsciously grades a patient as slightly better than they actually are. They do it to be encouraging or because they confuse what a patient can do with what a patient safely does.
While this makes the patient feel good in the moment, it devastates your Value-Based Purchasing score. By artificially raising the starting line, you destroy your ability to show improvement at the finish line.
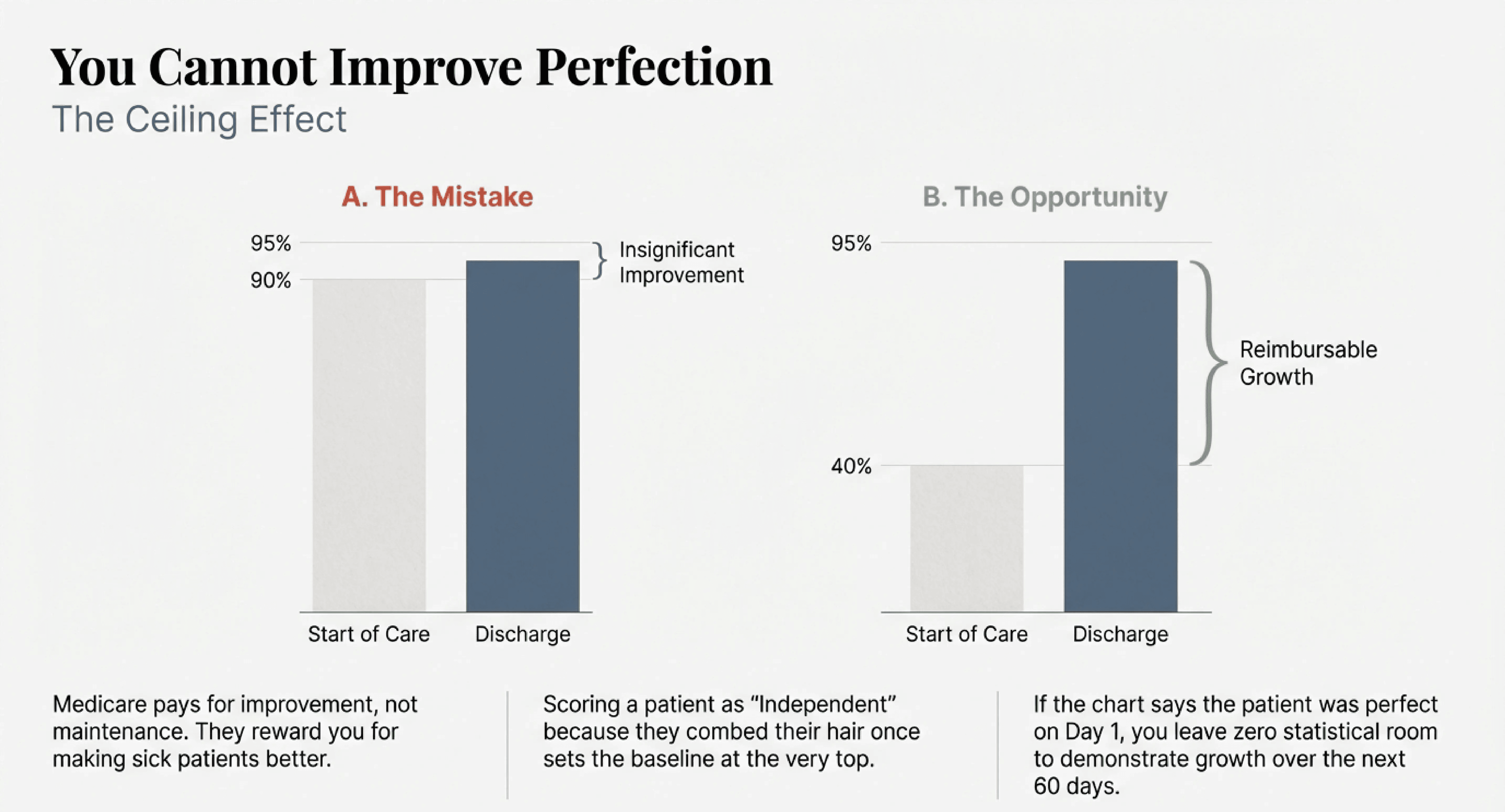
The Ceiling Effect
Medicare does not pay you for having healthy patients. They pay you for making sick patients better.
The Start of Care assessment establishes your baseline. If your nurse walks in and scores the patient as "Independent" in grooming because the patient managed to comb her hair once while sitting down, you have set your baseline at the very top.
You have left yourself zero room for growth.
Even if your team works miracles over the next 60 days, you cannot document improvement because the chart says the patient was perfect on day one. You have hit a statistical ceiling.
Capacity vs Performance
The root of this problem is often a misunderstanding of the OASIS definitions.
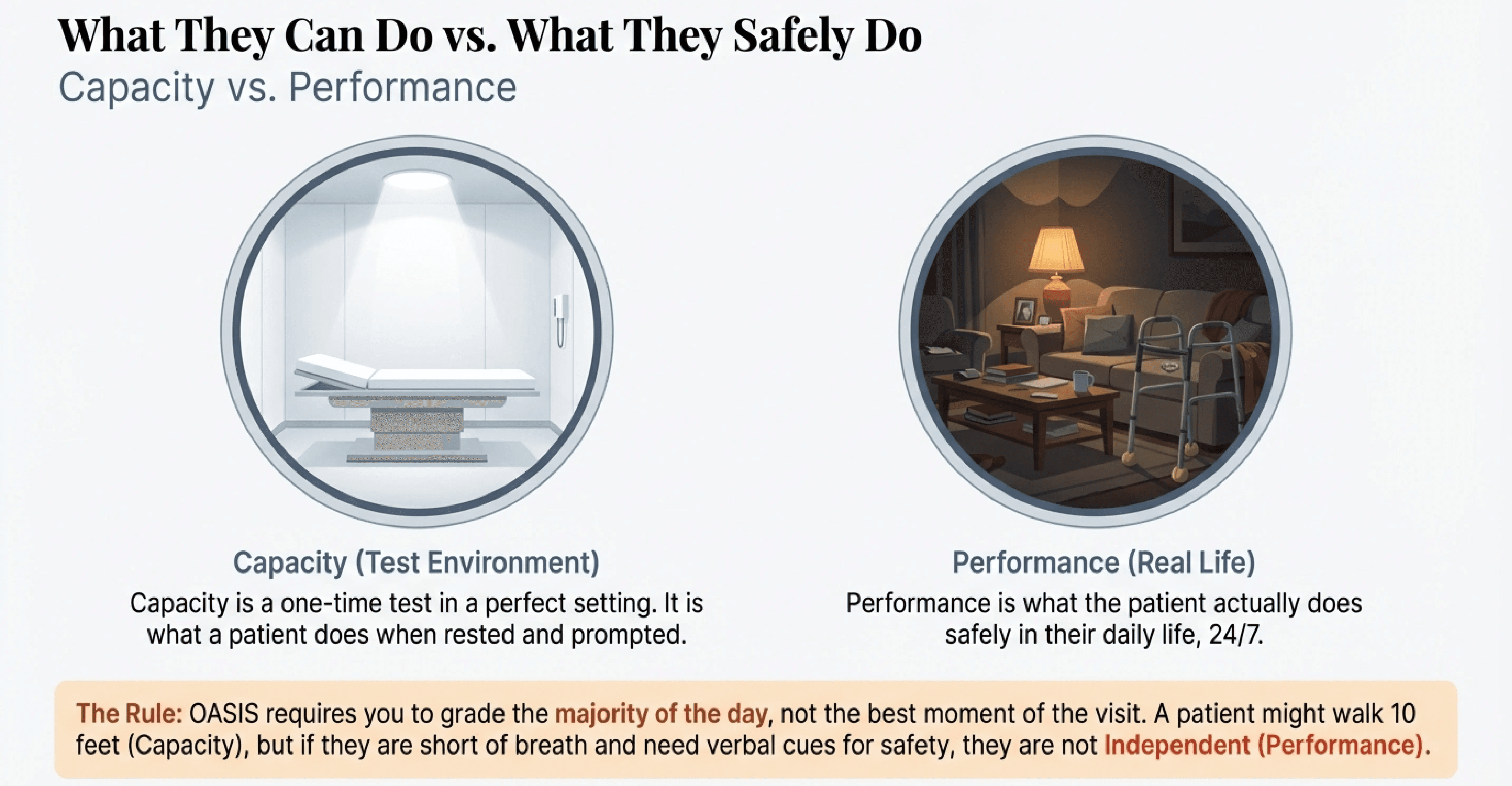
There is a massive difference between "Capacity" and "Performance."
Capacity is what a patient can do in a sterile testing environment when fully rested and prompted. Performance is what the patient actually does safely in their daily life, 24 hours a day.
Your "nice" nurse tends to chart Capacity. She sees the patient walk 10 feet with a walker and charts "Ambulation Improvement." She ignores the fact that the patient was short of breath, needed verbal cues for safety, and sat down immediately afterward.
She charts the best moment of the visit. The OASIS requires you to chart the majority of the patient's day.
The Logic Conflict
This optimism rarely survives a deep data audit. The truth usually hides in the narrative.
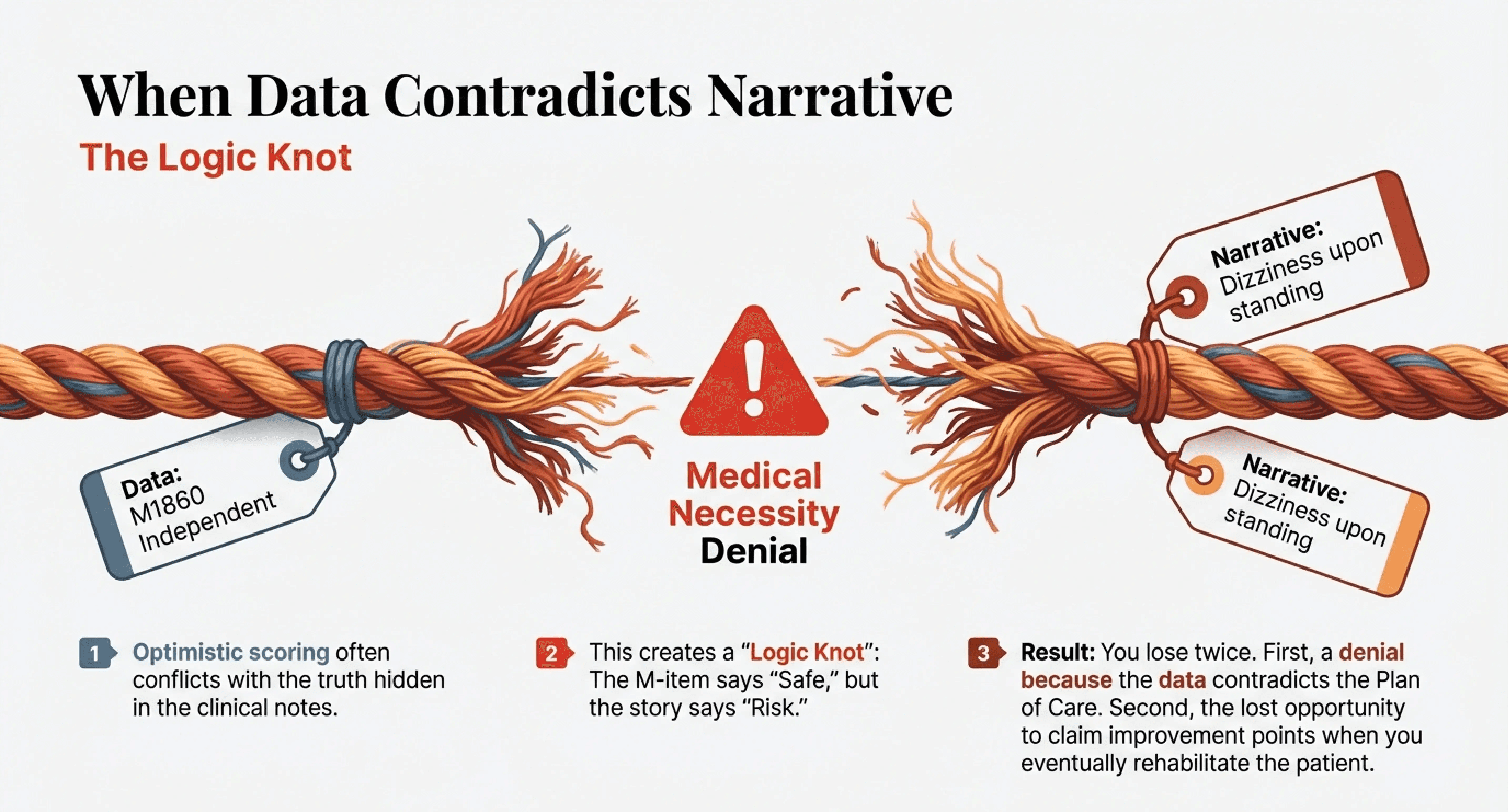
We often see charts where the M-items paint a picture of a highly functional, independent senior. But the narrative text tells a different story.
The nurse selects "Independent" for Transferring. Yet in the clinical note, she writes, "Patient requires standby assist due to dizziness upon standing."
This is a logic conflict. The data point says "Safe." The story says "Risk."
When you submit that chart, you lose twice. First, you risk a medical necessity denial because the data contradict the Plan of Care. Second, you lose the opportunity to claim the "Transferring" improvement points when you eventually rehabilitate that patient.
Objectivity is the Antidote
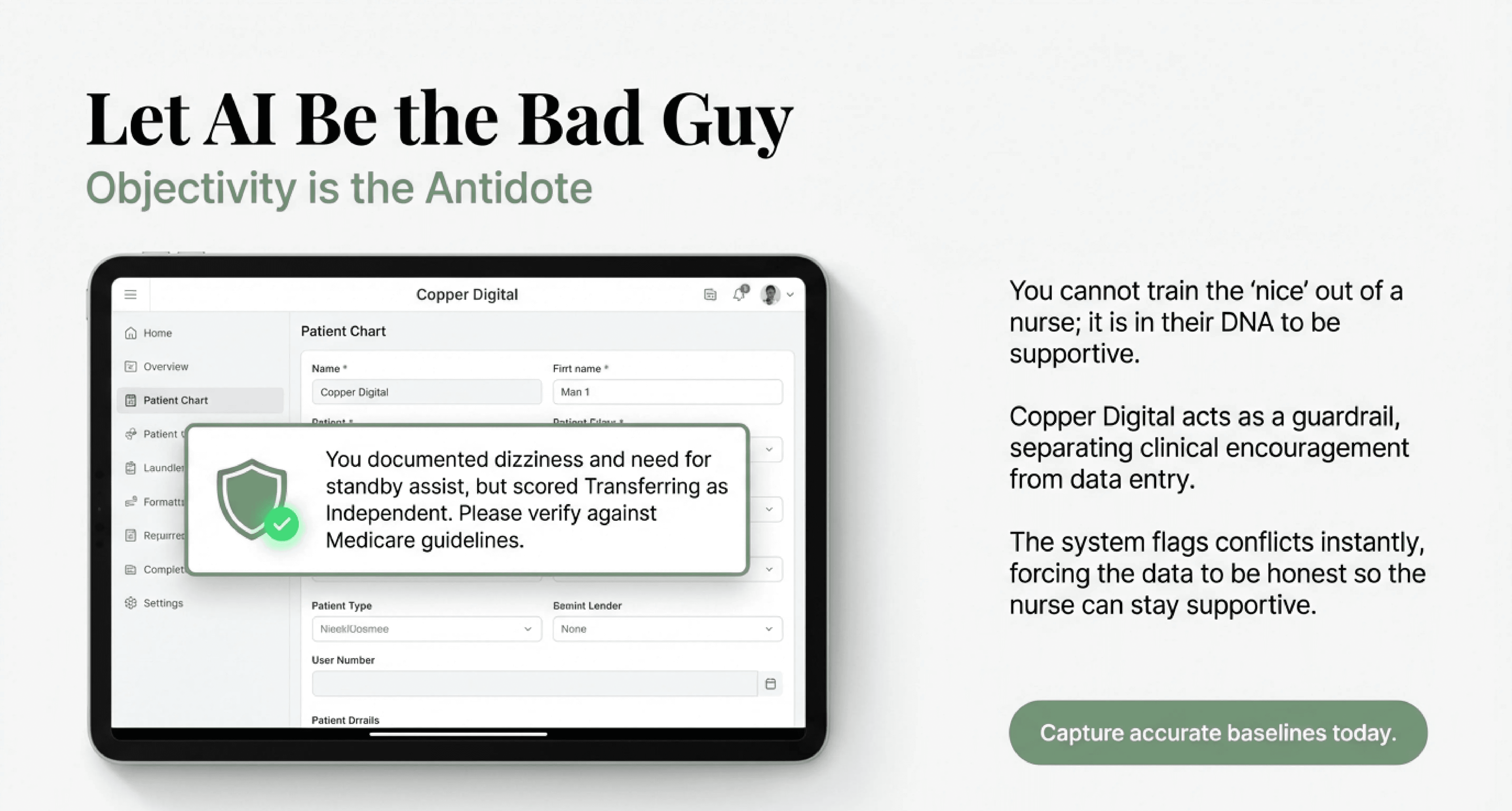
You cannot train the "nice" out of a nurse. It is part of their DNA to be supportive.
Instead, you need a guardrail that separates their clinical encouragement from their data entry.
This is where AI acts as the bad guy, so your nurse does not have to.
Copper Digital analyzes the entire chart before it is submitted. It reads the narrative where the nurse documented the dizziness. It compares that to the "Independent" score on the M-item.
It flags the discrepancy immediately.
The Prompt: "You documented that the patient has dizziness and requires standby assist. However, you scored Transferring as Independent. Medicare guidelines state this should be scored as a 1 or 2. Please verify."
This nudges the nurse back to reality. It forces them to grade based on the clinical facts rather than their emotional optimism.
Capture Your True Improvement
Accurate Start of Care charting feels harsh. It requires you to document every deficit, every struggle, and every limitation.
But that honesty is the only way to prove the value of your care.
If you want to maximize your reimbursement, you must stop fearing low scores at admission. Embrace them. The lower the accurate baseline, the higher the potential for improvement.
Let your nurses be nice to the patients. But force your data to be honest.
Start capturing accurate baselines today.
Frequently Asked Questions
1. Why does "nice" charting hurt my agency’s revenue?
Medicare Value-Based Purchasing (VBP) pays for improvement. Revenue is calculated based on the difference between the patient's status at admission (Start of Care) and their status at discharge. If a nurse "nicely" scores a patient as Independent at the start, they have set the baseline at 100%. You cannot improve from 100%. Therefore, the data shows zero improvement, and your agency loses the VBP performance points.
2. What is the difference between Capacity and Performance?
Capacity is what a patient can do in a controlled environment when focused and supervised (e.g., walking 10 feet for the nurse). Performance is what the patient actually does safely throughout the day and night when no one is watching. OASIS requires you to grade Performance. Grading Capacity creates a "false ceiling" that masks the patient's true deficits.
3. Does scoring lower on the OASIS mean my nurses are being critical?
No. It means they are being clinically accurate. Documenting a deficit (like "Unsafe to Ambulate") is not an insult to the patient; it is the justification for your skilled services. If a patient is scored as Independent, Medicare may argue that they do not need home health care at all, leading to a medical necessity denial.
4. How does Copper Digital fix the "Nice Nurse" problem?
You cannot easily train the natural empathy out of a caregiver. Copper Digital acts as an objective guardrail. It analyzes the narrative notes (where the nurse usually writes the truth about dizziness or fatigue) and compares them to the OASIS checkboxes. If the text says "Risk" but the checkbox says "Safe," the AI flags the contradiction instantly, prompting the nurse to correct the score before the chart is closed.
5. What is a "Logic Conflict" in documentation?
A Logic Conflict occurs when two data points in the same chart contradict each other. For example, if a nurse marks M1860 (Ambulation) as "Independent" but also documents "Shortness of breath at rest" in M1400. It is clinically impossible to be independent in walking if you cannot breathe while sitting. Auditors use these conflicts to deny claims.
6. Will correcting these scores negatively impact my Star Rating? Actually, the opposite is true. While your admission scores will likely drop (showing higher acuity/sickness), your improvement scores will rise significantly because you are finally capturing the true delta between admission and discharge. High improvement scores drive high Star Ratings and maximum VBP reimbursement.

