Blog
Apr 15, 2026
The LUPA Problem: What Causes It, What It Costs, and How to Prevent It Before the Period Closes

Arvind Sarin, CEO& Chairman of Copper Digital

Most agencies that track their LUPA rate treat it as a clinical operations metric. They look at it quarterly, note whether it went up or down, and move on. What they are not doing is tracking it the only way that actually changes it: in real time, by patient, by period, before the window closes.
By the time a LUPA shows up on a remittance advice, there is nothing left to do. The payment period has closed, the visit threshold was not met, and the agency is receiving a per-visit rate instead of the full episode payment. That difference is not recoverable through an appeal. It is not a billing error. It is the correct payment for what the claim reflects, and the only moment when it could have been prevented was sometime before the last day of the period.
LUPA is one of the most preventable revenue losses in home health, and it is preventable specifically because the threshold is not a surprise. Under PDGM, the minimum visit count for each 30-day payment period is determined by the clinical grouping at the start of that period. The number is knowable on day one. Tracking against it throughout the period and acting before it closes is a scheduling and coordination function. The agencies that have built that function are systematically eliminating a cost that most agencies have accepted as a normal feature of home health operations. It is not normal. It is preventable. This post explains exactly how, and connects the LUPA prevention workflow to the broader scheduling automation capabilities that address the same operational gaps.
What LUPA Actually Is Under PDGM
The Low Utilization Payment Adjustment is a payment reduction that applies when a home health agency delivers fewer visits in a 30-day payment period than the minimum threshold established for that patient's clinical grouping. Instead of receiving the full PDGM episode payment for that period, the agency receives a per-visit payment for each visit that was actually delivered.
Under the Patient-Driven Groupings Model, PDGM, each 30-day period is assigned to one of 432 Home Health Resource Groups based on five factors: the timing of the period within the episode (early or late), the clinical grouping of the primary diagnosis, functional impairment level, comorbidity adjustment, and admission source. Each HHRG has a specific LUPA threshold, the minimum number of visits required to receive the full payment for that grouping.
LUPA thresholds under PDGM range from two visits to six visits per 30-day period depending on the HHRG. For the majority of clinical groupings, the threshold is two to four visits. For certain high-complexity groupings, particularly those in the musculoskeletal and neurological categories, the threshold can be higher.
Why LUPA thresholds vary by HHRG CMS designed PDGM so that the LUPA threshold for each grouping approximates the typical visit utilization pattern for patients in that clinical category. Groupings with patients who typically receive fewer visits have lower thresholds. Groupings with patients who typically receive more visits have higher thresholds. An agency that consistently falls below threshold in high-utilization groupings is either underserving patients in those categories or experiencing operational gaps that are allowing visits to fall off without being replaced. |
What LUPA Costs in Real Terms
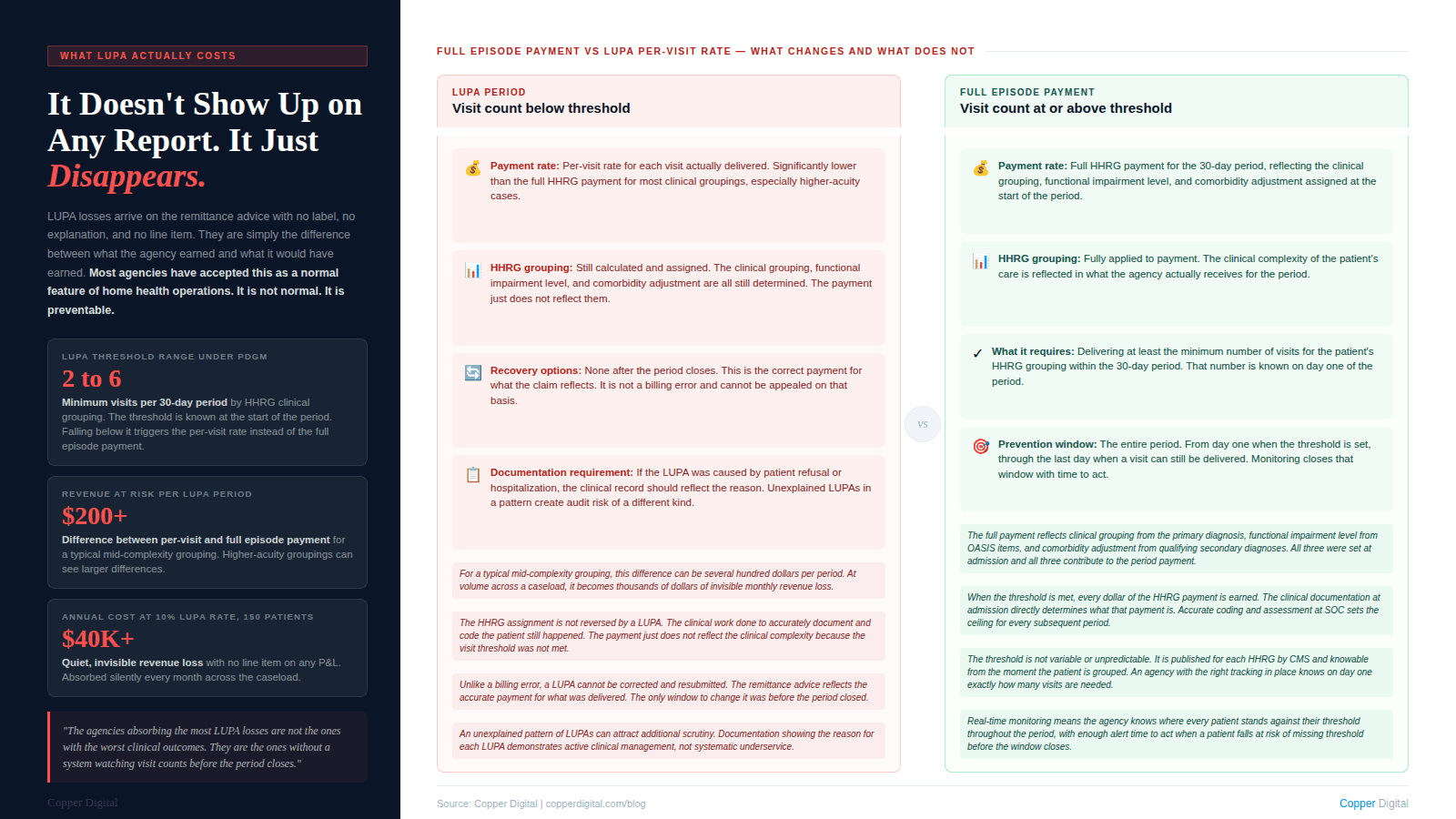
The financial impact of a LUPA is straightforward to calculate but rarely calculated by the agencies absorbing it. When a payment period triggers a LUPA, the agency receives a per-visit payment rather than the full HHRG payment. The per-visit rate is substantially lower than the full period payment for most clinical groupings, particularly those with higher acuity and complexity.
The revenue difference varies by HHRG, but across most clinical groupings the LUPA per-visit payment represents a fraction of what the full period payment would have been. For a mid-complexity patient in a typical grouping, a single LUPA period can mean a revenue loss of several hundred dollars compared to what the agency would have received had the threshold been met.
That number multiplies quickly at volume. An agency managing 150 active patients and experiencing a LUPA rate of 10 percent, which is within the range reported by many community-based agencies, is absorbing LUPA losses on 15 payment periods every 30 days. At an average revenue difference of a few hundred dollars per period, the annual cost can reach into the tens of thousands of dollars. It does not appear as a line item on any report. It appears only as the difference between what the agency earned and what it would have earned if the visits had been delivered.
The agencies absorbing the most LUPA losses are not the ones with the worst clinical outcomes. They are the ones without a system watching visit counts before the period closes. The threshold is knowable. The problem is preventable. |
The Four Scenarios That Generate LUPAs
LUPA does not happen randomly. It clusters around a small number of operational scenarios that appear consistently across agencies of different sizes and clinical mixes. Understanding which scenarios produce the most LUPAs at your agency is the first step toward building a prevention workflow that actually addresses the root cause.
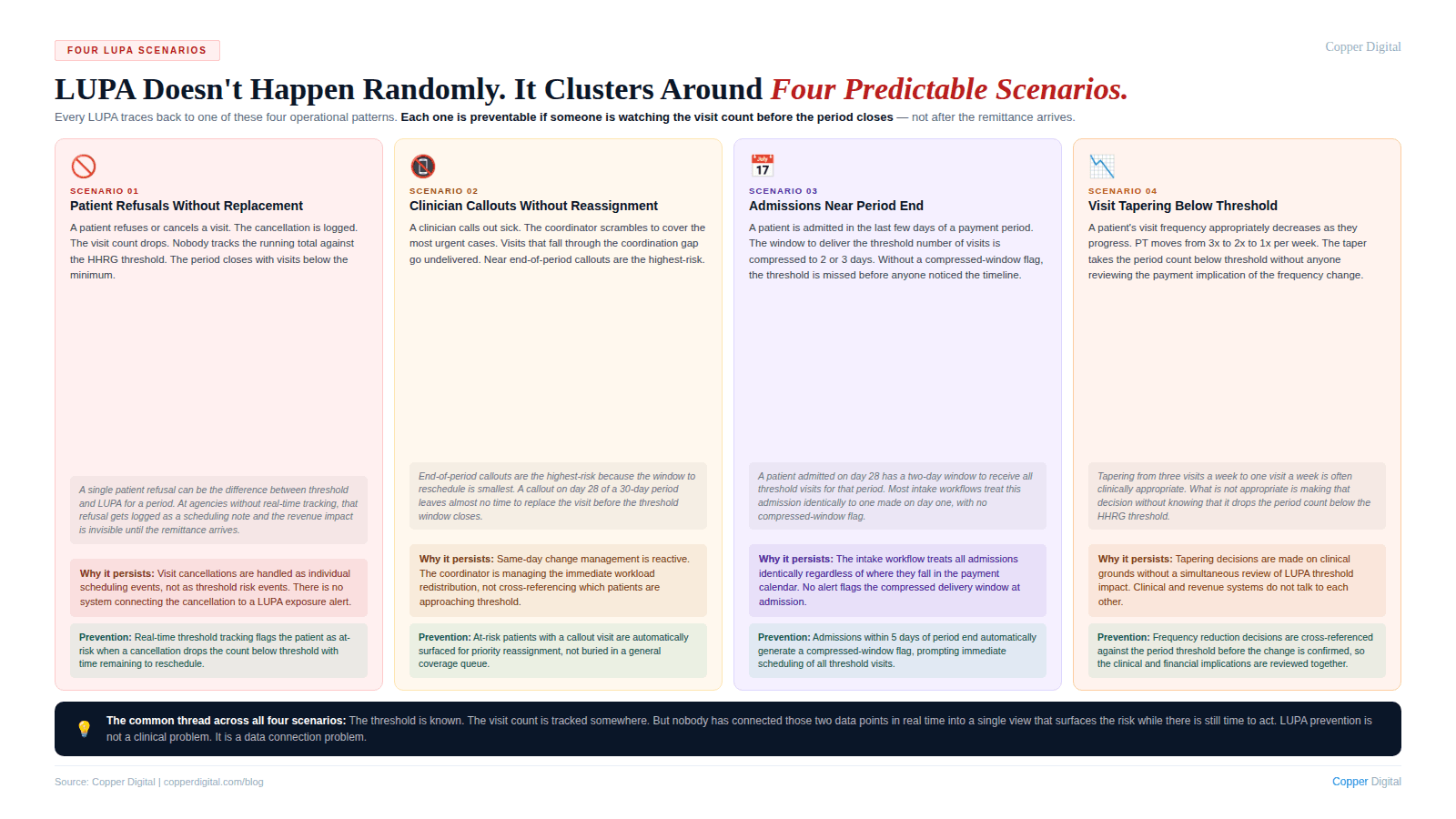
Scenario 1: Patient refusals and cancellations without replacement
The most common source of LUPAs is visits that were scheduled but not delivered because the patient refused or cancelled. A patient who refuses two visits in the second half of a 30-day period can easily push the visit count below threshold if nobody is tracking the running total and acting to recover the visits. The visit cancellation gets logged. The count drops. The period closes. Nobody noticed.
The distinction between patient refusals that were genuinely unrecoverable and patient refusals that were followed by no recovery attempt is important from a clinical standpoint. When a patient refuses a visit, the clinical record should reflect the refusal and the follow-up. From a revenue standpoint, the question is whether the agency attempted to reschedule within the period or simply accepted the gap.
Scenario 2: Clinician callouts without visit reassignment
When a clinician calls out sick or is otherwise unavailable, the coordination challenge of redistributing her caseload across other available clinicians is one of the most operationally taxing events in home health. The visits that get rescheduled are the ones the coordinator actively manages. The visits that fall through the gaps are the ones that eventually become LUPAs. This is the same same-day change management problem described in our post on scheduling automation. Missed visits from clinician callouts are particularly likely to push patients below threshold when the callout happens near the end of a payment period.
Scenario 3: Patients admitted near the end of a period
When a patient is admitted in the last few days of an early or late period, the available window for visit delivery is compressed by the calendar. A patient admitted on day 28 of a 30-day period has two days in that period, regardless of clinical need. If the threshold is two visits, the agency must deliver both visits in that window or trigger a LUPA for a period that barely existed. Many agencies do not have a process for identifying these compressed-window admissions and ensuring that the threshold is met within the narrow timeline available.
Scenario 4: Gradual visit tapering without threshold awareness
As patients progress clinically toward discharge, visit frequency naturally decreases. Physical therapy moves from three times a week to twice a week to once a week. Skilled nursing visits taper similarly. In many cases, this tapering is clinically appropriate. In some cases, the taper takes the visit count below threshold without anyone realizing it. A patient who was receiving four visits per week and has tapered to one visit per week in the final two weeks of a period may be below threshold before the tapering decision was ever reviewed against the payment implications.
Why Most Agencies Discover LUPAs Too Late
The structural reason LUPA prevention is so difficult at most agencies is that the information needed to prevent it, which visits have been delivered this period for which patients, is spread across multiple systems and is not synthesized into a real-time per-patient view that anyone is looking at proactively.
The billing system tracks completed visits against billing codes. The scheduling system tracks scheduled and completed visits against a calendar. The clinical record tracks visits against plan of care frequency requirements. None of these systems, in most agency technology stacks, is tracking visits against the LUPA threshold for the current payment period on a per-patient basis in real time.
What coordinators and supervisors end up doing is a manual reconciliation that nobody has time to do thoroughly: pulling visit counts from the EMR, cross-referencing against the PDGM HHRG assignment, calculating the remaining visits needed before the period closes, and identifying which patients are at risk. At a caseload of 50 to 100 active patients in various stages of their episodes, this is not a calculation that gets done accurately on a daily basis by hand.
The result is that most agencies discover their LUPAs on the remittance advice, at which point the payment period has already closed. The discovery happens after the fact, the number gets logged somewhere, and the agency moves on to the next month's remittance with no systemic change.
LUPA is not discovered at the bedside or in the clinical record. It is discovered on the remittance advice, weeks after the window to prevent it has closed. That timing gap is where prevention happens, and it requires a system watching the right number in real time. |
The LUPA Prevention Workflow
Preventing LUPAs requires exactly one thing: knowing which patients are approaching the threshold before the period closes and having enough time to act. That is a deceptively simple statement, but implementing it requires several connected components that most agencies do not have in place simultaneously.
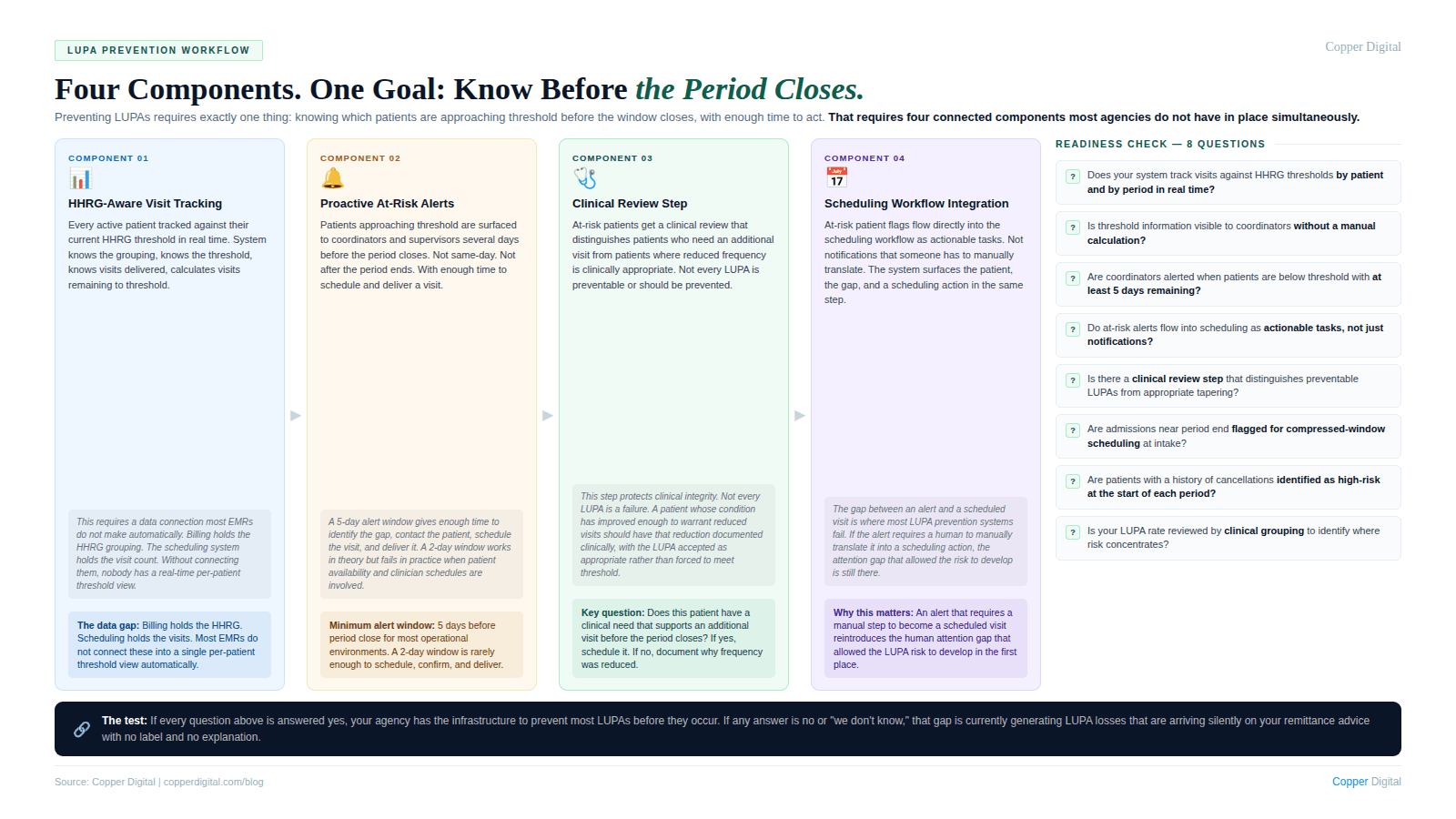
Component 1: HHRG-aware visit tracking by period
Every active patient should be tracked against their current HHRG threshold in real time throughout the payment period. This means the system knows the HHRG assignment for each patient, knows the LUPA threshold for that HHRG, knows how many visits have been delivered in the current period, and can calculate how many visits remain before threshold is met. This is a data connection between the billing system (which holds the HHRG assignment) and the scheduling and visit documentation systems (which hold the visit counts). Most EMRs do not make this connection automatically.
Component 2: Proactive at-risk patient identification
Several days before a payment period closes, every patient who has not yet met their HHRG threshold should be surfaced to the care coordinator or clinical supervisor. Not after the period closes. Not on the last day when there is no realistic time to schedule and deliver an additional visit. Several days before, when there is still a scheduling window to act.
The threshold for what counts as several days varies by agency size and scheduling complexity. For most agencies, a 5-day alert window gives enough time to identify the gap, contact the patient, schedule the visit, and deliver it before the period closes. A 2-day alert window is generally not enough.
Component 3: Clinical review of at-risk patients
Not every patient who is approaching threshold needs an additional visit purely for revenue reasons. Some patients are legitimately at a point in their care where reducing visit frequency is clinically appropriate. The LUPA prevention workflow needs a clinical review step that distinguishes between patients who need an additional visit because their care plan supports it and patients who have reached a clinical plateau where additional visits would not be justified.
This clinical review is not a rubber stamp. It is a genuine question: does this patient have a clinical need that supports an additional visit before the period closes? For patients who do, the visit should be scheduled. For patients who do not, the LUPA may be clinically appropriate and the focus should shift to ensuring the clinical record accurately reflects why visit frequency was reduced.
Component 4: Coordination with the scheduling workflow
At-risk patients identified through the LUPA prevention workflow need to be scheduled and delivered within the remaining period window. This is where the connection to the broader scheduling system matters. An at-risk patient flag that generates a notification but does not flow into the scheduling workflow requires someone to manually act on that notification, which reintroduces the human attention gap that allowed the LUPA risk to develop in the first place. The scheduling automation logic that surfaces LUPA at-risk patients as scheduling tasks, rather than as alerts someone has to translate into scheduling actions, is the component that converts a monitoring system into a prevention system.
LUPA and Clinical Quality: The Connection That Gets Missed
LUPA prevention is almost always framed as a revenue protection function. That framing is accurate but incomplete. A payment period that triggers a LUPA also means a patient received fewer visits than their clinical grouping anticipated. For many patients, that visit shortfall is clinically neutral because their condition improved and the reduced visits reflected appropriate tapering. For some patients, it reflects a gap in care.
The clinical and financial signals often point in the same direction. A patient who was receiving regular wound care visits and experienced a LUPA period because two visits were cancelled and not rescheduled may also have experienced a gap in wound monitoring that had clinical consequences. A patient whose visit frequency tapered below threshold in the final weeks of the period may have benefited from the visits that were not delivered.
Agencies that build LUPA prevention workflows often discover that the same patients who are at LUPA risk are also the patients whose care coordination has been least consistent. Addressing the operational gaps that generate LUPAs tends to improve both the financial picture and the clinical trajectory of the affected patients.
LUPA Risk by Clinical Grouping: Where to Focus First
LUPA risk is not evenly distributed across a caseload. It clusters in specific clinical groupings and patient types based on the interaction between threshold levels, typical visit patterns, and the operational challenges of delivering consistent visits to those patients.
Groupings with higher thresholds
Clinical groupings with LUPA thresholds of four or more visits per period have less margin for visit shortfalls. A grouping with a threshold of four requires four visits in thirty days. One patient refusal and one clinician callout in the same period can push the count to two visits delivered, which is below threshold by two. Agencies with significant caseloads in musculoskeletal, neurological, or other higher-threshold groupings should prioritize those patients in their LUPA monitoring workflow.
Patients in the late-episode period
In PDGM, the late period payment is generally lower than the early period payment because the model anticipates that clinical intensity decreases as patients recover. LUPA risk in late-episode periods can be higher because visit tapering is often appropriate at that stage, and the line between clinically appropriate tapering and below-threshold underservice is easy to cross without realizing it. Late-episode patients approaching their second or third 30-day period benefit most from proactive threshold monitoring.
Patients with a history of cancellations or refusals
Clinical history data on visit refusals and cancellations by patient is one of the most actionable signals in LUPA prevention. A patient who refused or cancelled multiple visits in a prior period is statistically more likely to do so in the current period. Proactive outreach at the start of a new period for patients with a cancellation history, confirming the visit schedule and addressing barriers to compliance, reduces the LUPA risk before it develops rather than responding after visits have already been missed.
What to Do When a LUPA Is Unavoidable
Despite best prevention efforts, some LUPAs will occur. A patient who is hospitalized mid-period, a patient who moves out of the service area, or a patient who makes an autonomous clinical decision to refuse care may trigger a LUPA regardless of how well the agency manages its prevention workflow. When a LUPA is unavoidable, the focus shifts to documentation.
A LUPA that is documented as the result of patient refusal, patient hospitalization, or another legitimate clinical circumstance is different from a LUPA that is simply unexplained. The clinical record for an unavoidable LUPA period should reflect: what visits were attempted and refused, the clinical reason for the patient's refusal or unavailability, what follow-up was attempted, and whether the physician was notified of the visit shortfall.
This documentation does not change the payment. The LUPA rate is applied regardless of the reason. But it does protect the agency from a more significant audit concern: a pattern of LUPAs with no clinical explanation that could suggest underservice rather than appropriate clinical management.
LUPA and the HHVBP connection A LUPA period where visits were not delivered may also affect HHVBP outcome measures if the missed visits corresponded to clinical monitoring or therapeutic interventions that would have contributed to measured functional improvement. Agencies managing their LUPA rate are often simultaneously managing their HHVBP performance, because the same operational gaps that allow LUPAs to develop are frequently the gaps that allow patients to progress less than they would have with consistent visit delivery. |
A LUPA Prevention Readiness Checklist
Use this checklist to evaluate whether your agency has the components in place to prevent LUPAs before they occur rather than discovering them after the period closes.
Data and visibility
Does your system track visit counts against HHRG thresholds by patient and by period in real time?
Is LUPA threshold information visible to care coordinators and clinical supervisors without requiring a manual calculation?
Is there a report or dashboard showing all active patients who are currently below threshold with the number of days remaining in their period?
Proactive alerting
Are coordinators alerted when a patient is approaching LUPA threshold with enough time remaining to schedule and deliver an additional visit?
Is the alert window long enough to realistically act? At minimum five days before the period closes for most operational environments.
Does the alert flow into the scheduling workflow as an actionable task, or does it require a separate manual step to convert into a scheduled visit?
Clinical review
Is there a defined clinical review step for at-risk patients that distinguishes between patients who need additional visits and patients for whom reduced visit frequency is clinically appropriate?
When a LUPA is deemed clinically appropriate, is the rationale documented in the clinical record?
Pattern analysis
Is your LUPA rate tracked by clinical grouping and by patient type to identify where LUPA risk concentrates in your caseload?
Is patient-level cancellation and refusal history used to identify high-risk patients at the start of new periods?
Is LUPA rate reviewed in clinical and operations leadership conversations, not just in billing?
Copper Digital tracks visit counts against PDGM LUPA thresholds in real time, surfaces at-risk patients as scheduling tasks before the period closes, and connects the LUPA prevention workflow directly to your scheduling and care coordination process. Request a demo to see how this works for your agency. |
Related Reading

