Blog
Mar 2, 2026
Why Home Health Agencies Fail ADR and TPE Audits

Arvind Sarin

An Additional Documentation Request lands in your inbox. You have 45 days to pull the records, build a response, and submit documentation that convincingly demonstrates medical necessity for every visit under review. If you cannot, you face partial or full recoupment. If you miss the deadline, you waive your right to appeal.
Most home health agencies treat ADRs as paperwork fires. They scramble, pull charts, hope the documentation is sufficient, and often discover mid-response that the clinical record does not actually support what was billed. Not because the care was inappropriate, but because the documentation was never built to survive scrutiny.
The fix is not faster response time. The fix is documentation that is audit-ready before the ADR arrives. This post breaks down exactly what triggers ADRs and TPE audits, what CMS reviewers are looking for, the most common reasons agencies lose these reviews, and what a compliant documentation workflow actually looks like.
ADR vs. TPE: What Is the Difference
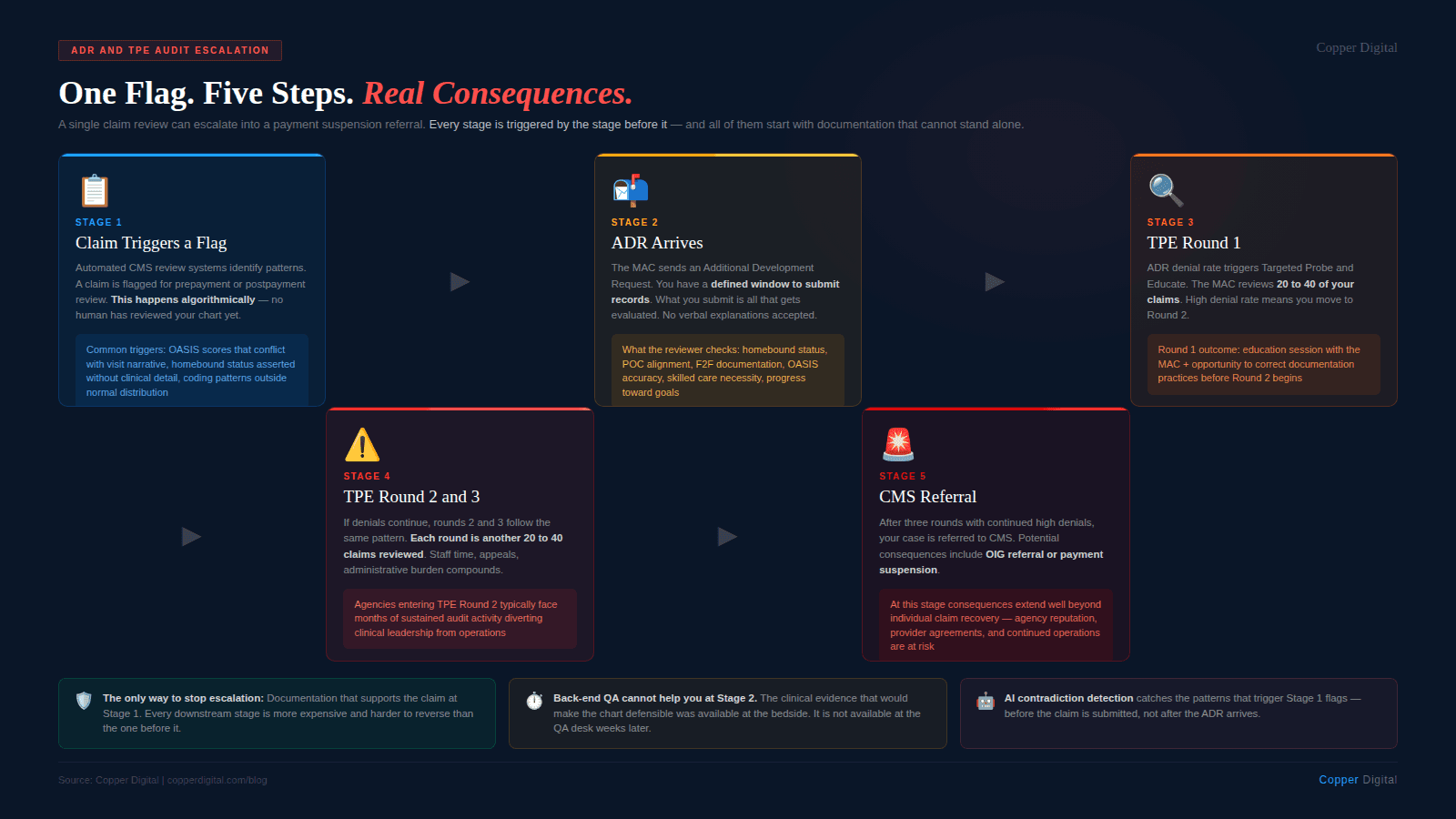
ADR (Additional Documentation Request): A request from a Medicare Administrative Contractor (MAC) or the Recovery Audit Contractor (RAC) for medical records supporting a specific claim. ADRs can be issued pre-payment (before the claim is paid) or post-payment (after the claim is already paid and potentially subject to recoupment). Home health ADRs are typically focused on individual claims and require a response within 45 days.
TPE (Targeted Probe and Educate): A CMS-directed program where MACs select providers with high claim error rates or billing patterns that suggest systemic problems, then review up to 40 claims across three rounds. TPE is designed to be educational — the MAC is supposed to offer feedback and give the agency an opportunity to correct errors — but repeated failures move a provider toward referral to the RAC or the OIG, which carries significantly higher stakes.
Both processes ultimately ask the same question: does your documentation prove that the patient was homebound, had a skilled nursing or therapy need, and received medically necessary care that was ordered by a physician and delivered as documented?
ADRs are not random. MACs use data analytics to identify patterns — high utilization, unusual diagnosis combinations, agencies with consistent OASIS accuracy issues. If you are being audited, there is likely a systematic reason. |
What Triggers an ADR or TPE Review
Understanding audit triggers is the first step toward prevention. The most common reasons a home health agency gets selected for review include:
High utilization outliers
Agencies whose episode utilization, number of visits per episode, or therapy thresholds fall significantly outside the MAC's regional norms are flagged automatically. This does not mean your care was inappropriate, but it means your documentation needs to be proportionally strong. If you are billing above regional norms, every visit needs to be clinically justified.
OASIS accuracy flags
CMS analyzes OASIS data for internal contradictions and statistical anomalies. If your agency's patients consistently show higher severity on admission and lower severity at discharge than expected for your patient population, that is a billing pattern flag. If your functional assessments in Section GG are inconsistent with your clinical narrative in your nursing notes, that is a documentation integrity flag. Both get attention.
New or recently growing agencies
Rapid growth in patient volume or billing is a common trigger. MACs pay attention to agencies that scale quickly, particularly in markets with known fraud history.
Face-to-face and homebound documentation deficiencies
Face-to-face encounter requirements and homebound status are consistently among the top reasons for ADR failure. If these are routinely incomplete or boilerplate in your records, you are at elevated risk.
Specific diagnosis patterns
Certain diagnosis codes and PDGM groupings are subject to higher scrutiny. Agencies billing heavily in high-reimbursement PDGM categories without proportionally detailed clinical documentation attract review.
The Five Most Common Reasons Agencies Lose ADR Reviews
Based on MAC guidance, CMS audit findings, and industry reporting, these are the documentation failures that result in the most recoupment:
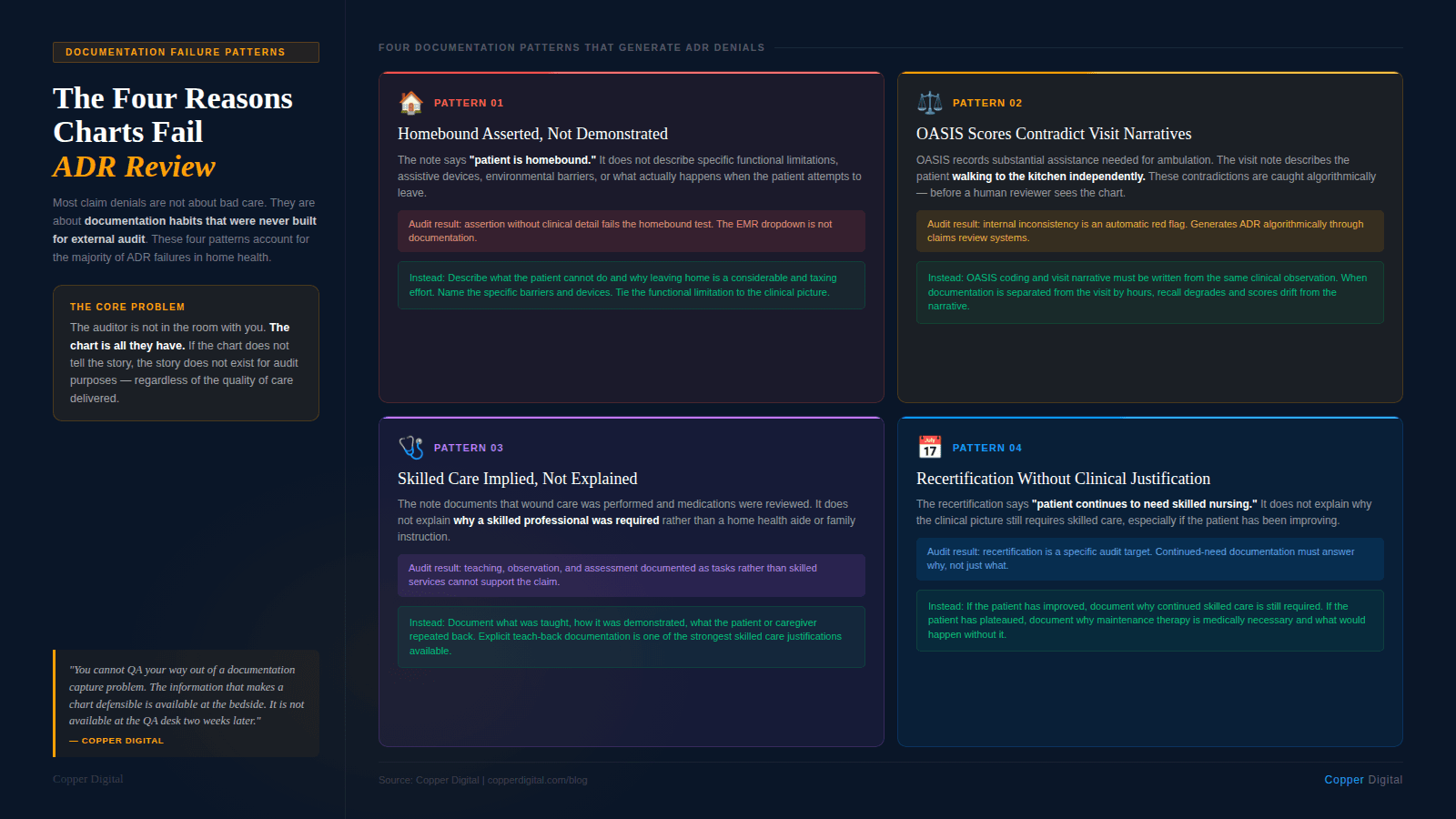
1. Homebound status is asserted but not demonstrated
Homebound status is a legal threshold, not a clinical opinion. The record must show that leaving home requires a considerable and taxing effort. A checkbox or a single sentence saying the patient is homebound is not sufficient. The documentation needs to describe the specific physical or medical condition that makes leaving difficult, the type of assistance required, and whether the patient does leave home and how often and why.
See our earlier post on homebound status documentation for the exact language patterns that hold up under review.
2. Face-to-face documentation is missing, late, or inadequate
A face-to-face encounter must occur within 90 days before or 30 days after the start of a home health episode, and the documentation must demonstrate that the physician or allowed practitioner personally examined the patient and that the clinical findings support home health eligibility. A phone call does not qualify. A signed order without clinical findings does not qualify. A narrative that does not connect the examination findings to the home health need does not qualify.
This is one of the highest-frequency ADR failure points and one of the most preventable.
3. The care plan is not physician-signed or is not reflected in the clinical notes
Every visit must connect to an active, signed plan of care. If your nurses are delivering care that drifts from the documented plan, or if the plan was not signed before the episode period started, those visits become indefensible. Auditors look for alignment between the 485, the OASIS, the nursing notes, and the therapy documentation. Gaps between them are red flags.
4. Skilled need is not documented, only tasks
Nursing notes that describe vital signs taken, wound dressed, patient educated without connecting those tasks to a skilled nursing judgment or clinical decision are not sufficient to establish skilled need. CMS reviewers are looking for documentation of why a skilled nurse was required for this visit, not just what the nurse did. The clinical complexity, the patient's condition, and the teaching necessity all need to be present in the record.
5. OASIS is internally inconsistent
An OASIS that scores a patient as having significant functional limitations but whose nursing notes describe the patient ambulating independently around the home will not survive review. Neither will an OASIS that flags respiratory compromise but whose clinical narrative never references respiratory status. Auditors cross-check these documents, and inconsistencies raise questions about the validity of the assessment as a whole.
The most expensive audit failure is not fraud. It is a care record that was accurate in the nursing notes but never built to demonstrate medical necessity. The care was appropriate. The documentation just could not prove it. |
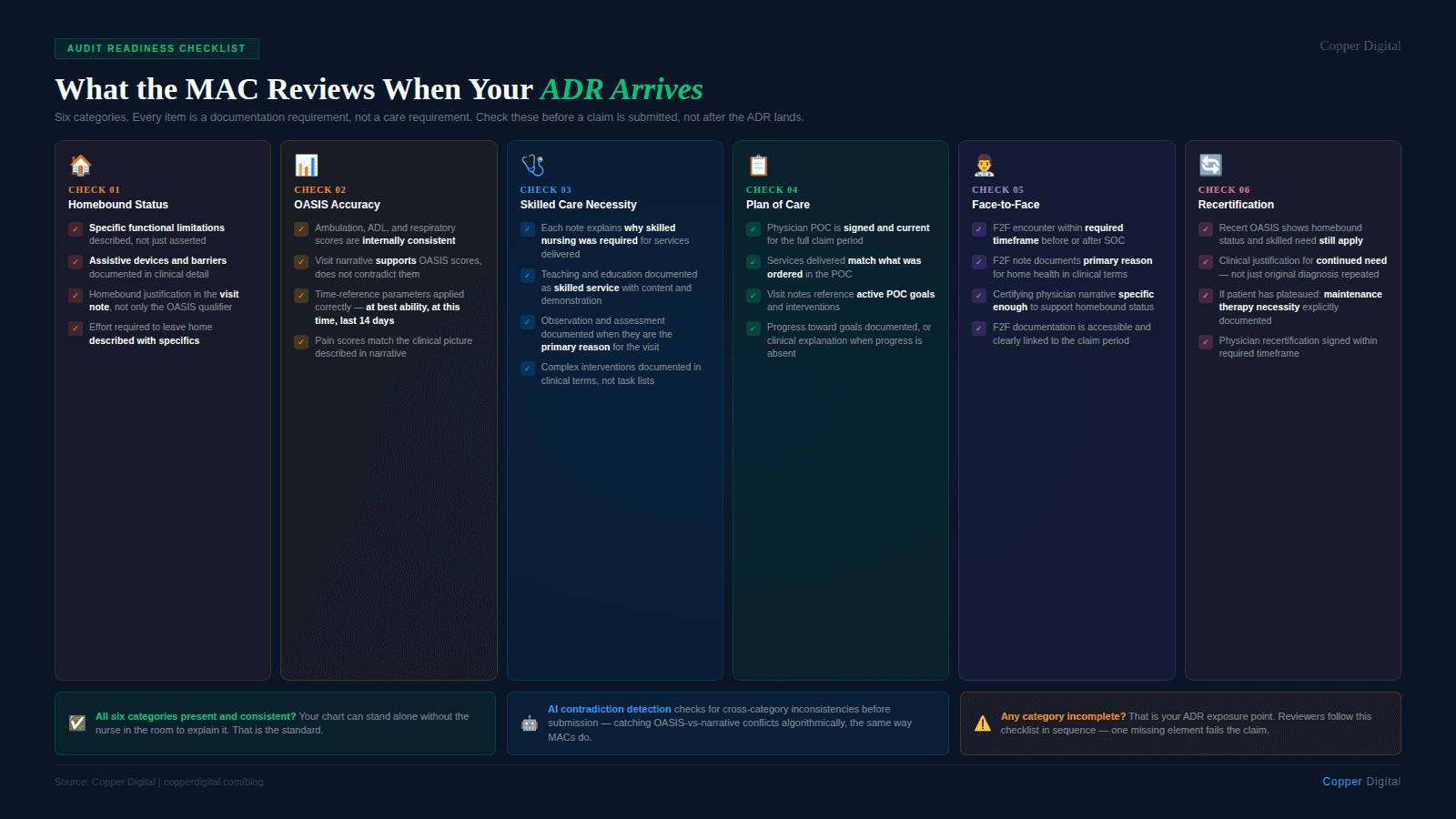
Building Your ADR Response: What Goes In the Package
When an ADR arrives, you are typically asked to submit the complete medical record for the claim period under review. What that means in practice:
The signed physician order and plan of care (CMS-485) for the episode in question
The face-to-face encounter documentation, including the clinical findings and the certifying statement
The complete OASIS assessment, including all sections relevant to homebound status, functional limitations, and primary diagnosis
All visit notes for the episode, signed and dated by the clinician who performed the visit
Therapy evaluation and re-evaluation notes if therapy visits are part of the claim
Any home health aide supervisory notes if aide visits are included
Discharge OASIS or transfer documentation if the episode has ended
Any physician communication, including verbal orders, signed communication, and progress notes if available
The package needs to be organized, complete, and submitted on time. Missing documents cannot be added after submission in most appeal pathways. Documents that arrive after the deadline are typically not considered.
Writing the cover letter
The cover letter is your opportunity to make the case affirmatively before the reviewer reads the records. It should not be generic. It should specifically address homebound status, skilled need, and medical necessity for this patient, referencing specific pages in the record that support each element. A strong cover letter does not replace good documentation — but it guides the reviewer toward the evidence and makes it easier to find.
The TPE Process: What to Expect Across Three Rounds
TPE moves in rounds. In Round 1, the MAC reviews up to 20 claims. If the error rate is unacceptably high, Round 2 follows with up to 20 more. If errors persist, Round 3 covers up to 40 claims. After three rounds without improvement, the agency is referred for further action.
Between rounds, the MAC is required to offer education. This is not optional and should not be ignored. The education session typically identifies the specific documentation deficiencies the MAC found. Those deficiencies should drive immediate protocol changes before the next round begins.
Agencies that use TPE feedback to fix systemic issues before Round 2 typically see significant improvement. Agencies that treat it as a compliance event rather than a clinical operations signal continue to fail.
What the MAC feedback actually tells you
MAC feedback after a TPE round is specific. It will tell you which claim types had errors, what documentation elements were missing or insufficient, and what the error rate was. Treat this as a free audit of your documentation system. Every finding maps to a process that needs to change.
What Audit-Ready Documentation Actually Looks Like
The goal is not to document for auditors. The goal is to document the clinical reality so completely and clearly that an auditor reading the record four months after the visit can understand exactly what the patient's condition was, why skilled nursing was needed, and what was done and why. A record that achieves this is simultaneously a good clinical record and an audit-ready one.
Homebound language that holds up
Instead of: "Patient is homebound due to diagnosis."
Use: "Patient requires maximum assistance for ambulation and cannot navigate stairs without two-person assist. Leaving home requires arranging transportation assistance, use of wheelchair, and significant recovery time. Patient leaves home only for medical appointments, approximately once per month, with assistance from daughter. Taxing effort documented per physician order and patient report."
Skilled need that establishes necessity
Instead of: "Nurse visited, assessed vitals, educated on medications."
Use: "Patient demonstrated subtherapeutic INR of 1.8 on this visit despite previous Warfarin adjustment. Clinical judgment required to assess for signs of thromboembolism, contact physician for dose modification order, and educate patient on diet-drug interactions contributing to INR instability. Skilled nursing required for medication management complexity and for patient safety monitoring given anticoagulation risk."
OASIS that matches the chart
Every OASIS response must be defensible by the clinical record around it. Before finalizing any OASIS assessment, QA should run a cross-check: does the GG functional status align with the nursing notes? Does the respiratory status align with the vital sign documentation? Does the cognitive status align with the therapy notes? These checks catch the contradictions that become recoupment.
How Documentation Automation Reduces ADR Risk
The most consistent driver of ADR failure is not clinician negligence. It is documentation that was completed under time pressure, hours after the visit, from memory. A clinician who saw six patients in a day, drove between each one, and is completing her OASIS at 9 p.m. is not going to produce the same quality record as one who documented in real time with contextual support.
This is what clinical documentation AI addresses. By reducing the documentation burden on field nurses, automating the extraction of clinical information from referral packets and H&P documents, and flagging internal inconsistencies in the OASIS before submission, AI-assisted documentation tools help agencies produce records that are more accurate, more complete, and more consistent — which is exactly what survives an ADR review.
Specifically, automated documentation workflows can: flag when homebound documentation language is insufficient before the claim is submitted, identify OASIS responses that contradict the clinical narrative, surface missing face-to-face documentation before the episode closes, pre-populate administrative fields from the referral so the nurse can focus her documentation time on clinical judgment, and generate a visit summary that connects each task to a skilled need. None of these replace clinical judgment. All of them protect the record that documents it. See how this works in our post on how Medicare bots find the errors humans miss.
Your ADR Response Checklist
Use this checklist when an ADR arrives. It will not substitute for a thorough record review, but it will keep you from missing the basics.
On receipt:
Note the response deadline immediately. 45 days from the date on the letter, not the date you received it.
Identify every claim number listed in the ADR. Each claim needs its own documentation package.
Assign a specific staff member to own the response. ADRs that get passed around lose time.
Chart review:
Confirm face-to-face documentation is present, dated within the required window, and contains clinical findings.
Confirm the signed 485 is in the record and covers the episode period.
Pull all visit notes. Confirm they are signed, dated, and clinically complete.
Cross-check the OASIS against the nursing notes for internal consistency.
Verify homebound status documentation includes specific functional description and effort required to leave.
Confirm skilled need is documented with clinical rationale, not just task description.
Submission:
Organize the package in the order the MAC specifies. Many MACs have required formats.
Write a cover letter that affirmatively makes the case for each element under review.
Keep a copy of everything submitted, with proof of submission and the date.
Calendar the decision deadline so you know when to expect a response and when the appeal window opens if you need it.
If You Lose the Initial Review: The Appeals Process
A denied ADR is not the end of the road. Medicare has a five-level appeals process for home health claims:
Level 1: Redetermination — MAC reviews the decision. Submit within 120 days of the initial determination. New evidence can be submitted.
Level 2: Reconsideration — Qualified Independent Contractor (QIC) reviews. Submit within 180 days of the redetermination notice.
Level 3: ALJ Hearing — Administrative Law Judge. Available if the amount in controversy meets the threshold (currently $180 or more per year). Submit within 60 days of the QIC decision.
Level 4: Appeals Council — Medicare Appeals Council reviews. Submit within 60 days of the ALJ decision.
Level 5: Federal Court — Available if the amount in controversy meets the federal court threshold. Submit within 60 days of the Appeals Council decision.
The most important thing to know about appeals: win rates improve significantly at the ALJ level compared to the MAC redetermination level. Many agencies give up after Level 1 or 2. If you have strong documentation and a legitimate claim, pursuing through Level 3 is often worth it.
Copper Digital helps home health agencies build documentation workflows that are compliant before the ADR arrives, not after. Our AI-assisted tools flag homebound documentation gaps, OASIS inconsistencies, and missing face-to-face documentation in real time, so your clinical record is defensible from the start. Request a demo to see how it works. |
Related Reading

