Blog
Apr 1, 2026
Verbal Orders in Home Health: What Counts, What Must Be Signed, and When

Arvind Sarin
Verbal orders are one of the most operationally significant and least formally understood elements of home health practice. They authorize clinical changes between plan of care cycles, keep care moving when documentation timelines cannot wait, and make home health's flexible care model possible. They are also one of the most consistent sources of documentation problems when the process for managing them is informal or inconsistent.
Most home health nurses understand that verbal orders exist and that they need to be followed up with a written order. Fewer understand what specific types of clinical changes require a verbal order, which orders must be signed before the next recertification, and what happens to a claim when verbal orders are missing or unsigned at audit. This post covers the mechanics of verbal orders in home health: what they authorize, what they require, and the documentation workflow that keeps them defensible. For the broader clinical record structure they sit within, see our post on the start of care visit and how the care plan and plan of care work together.
What a Verbal Order Actually Is
A verbal order in home health is a spoken authorization from a physician or allowed practitioner that permits a change to the patient's care outside of the formal plan of care signing cycle. The physician does not need to sign a document for the nurse to act on the order. The verbal authorization is sufficient to proceed with the clinical change immediately.
This is a meaningful distinction from hospital practice. In an inpatient setting, verbal orders are exceptions to the rule: the standard is written and signed orders for everything. In home health, verbal orders are a standard operating mechanism because the plan of care covers a 60-day certification period and clinical changes happen continuously between plan of care renewals. The verbal order system allows those changes to be authorized and documented without requiring the physician to sign a new plan of care every time a wound dressing changes or a medication dose is adjusted.
The verbal order creates a legally valid authorization for the clinical action. It must then be documented in writing by the nurse who received it and sent to the physician for signature. The written documentation of the verbal order becomes part of the patient's permanent medical record. The physician's signature on the written order confirms that the verbal authorization happened and that the physician is accountable for the order.
Who can give a verbal order A verbal order must come from the certifying physician or, in cases where the physician has authorized it, from another treating physician managing a specific aspect of the patient's care. Non-physician practitioners may give verbal orders within the scope of their practice and applicable state law, consistent with their collaborative agreements with the certifying physician. A verbal order cannot come from a home health agency staff member, a family member, or anyone other than a qualified licensed practitioner authorized to order home health services. |
What Types of Changes Require a Verbal Order
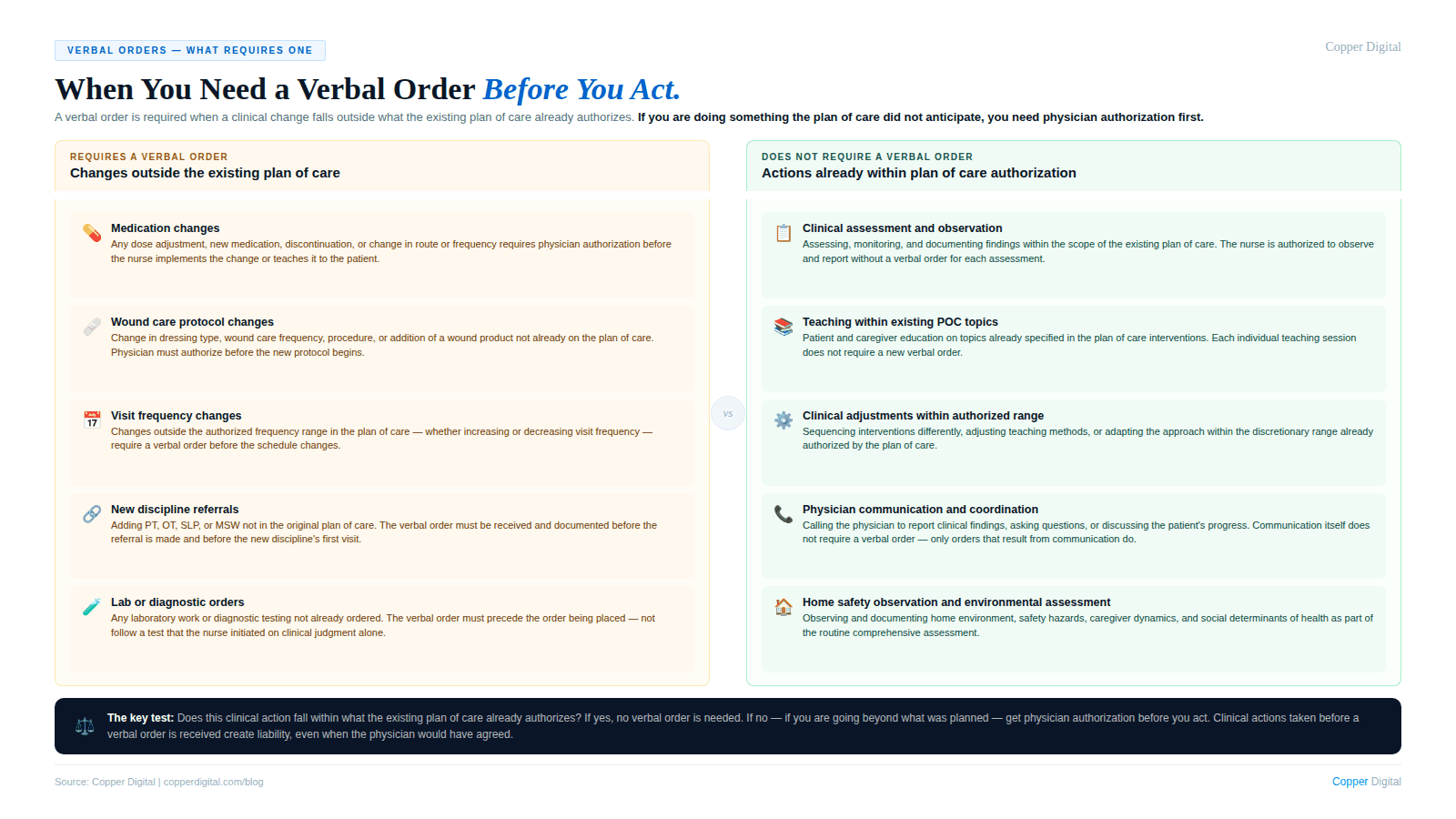
Not every clinical adjustment in home health requires a verbal order. Nurses have professional judgment latitude within the scope of what the plan of care already authorizes. A verbal order is required when a clinical change falls outside the existing plan of care authorization.
Changes that require a verbal order
Medication changes. Any change to a medication — dose adjustment, addition of a new medication, discontinuation of an existing medication, or change in route or frequency — requires a verbal order before the nurse implements the change and teaches it to the patient.
Wound care protocol changes. A change in the wound dressing type, the wound care frequency, the wound care procedure, or the addition of a wound care product not already on the plan of care requires a verbal order.
Frequency changes. If the visit frequency specified in the plan of care needs to increase or decrease, a verbal order is required. The plan of care specifies visit frequency as an authorized range. Changes outside that range require physician authorization.
New discipline referrals. If the nurse identifies a need for physical therapy, occupational therapy, speech therapy, or social work that was not part of the original plan of care, a verbal order is required before the referral can be made.
Lab or diagnostic orders. If the nurse identifies a clinical need for laboratory work or diagnostic testing not already ordered, a verbal order from the physician is required before the order can be placed.
New skilled nursing orders. If a new skilled nursing intervention not covered by the existing plan of care is clinically indicated, a verbal order is required before it can be documented as an authorized service.
Changes that do not require a new verbal order
Clinical assessments and observations documented in visit notes within the scope of the existing plan of care do not require verbal orders. The nurse is authorized to assess, monitor, and document as part of the ongoing skilled nursing service.
Teaching and education within the topics already specified in the plan of care interventions do not require verbal orders for each teaching session.
Clinical adjustments that fall within the discretionary range already authorized in the plan of care, such as adjusting teaching methods or sequencing interventions differently, do not require verbal orders.
A verbal order is required when a clinical change falls outside what the existing plan of care already authorizes. If you are doing something the plan of care did not anticipate, you need physician authorization before you do it. |
The Verbal Order Documentation Workflow
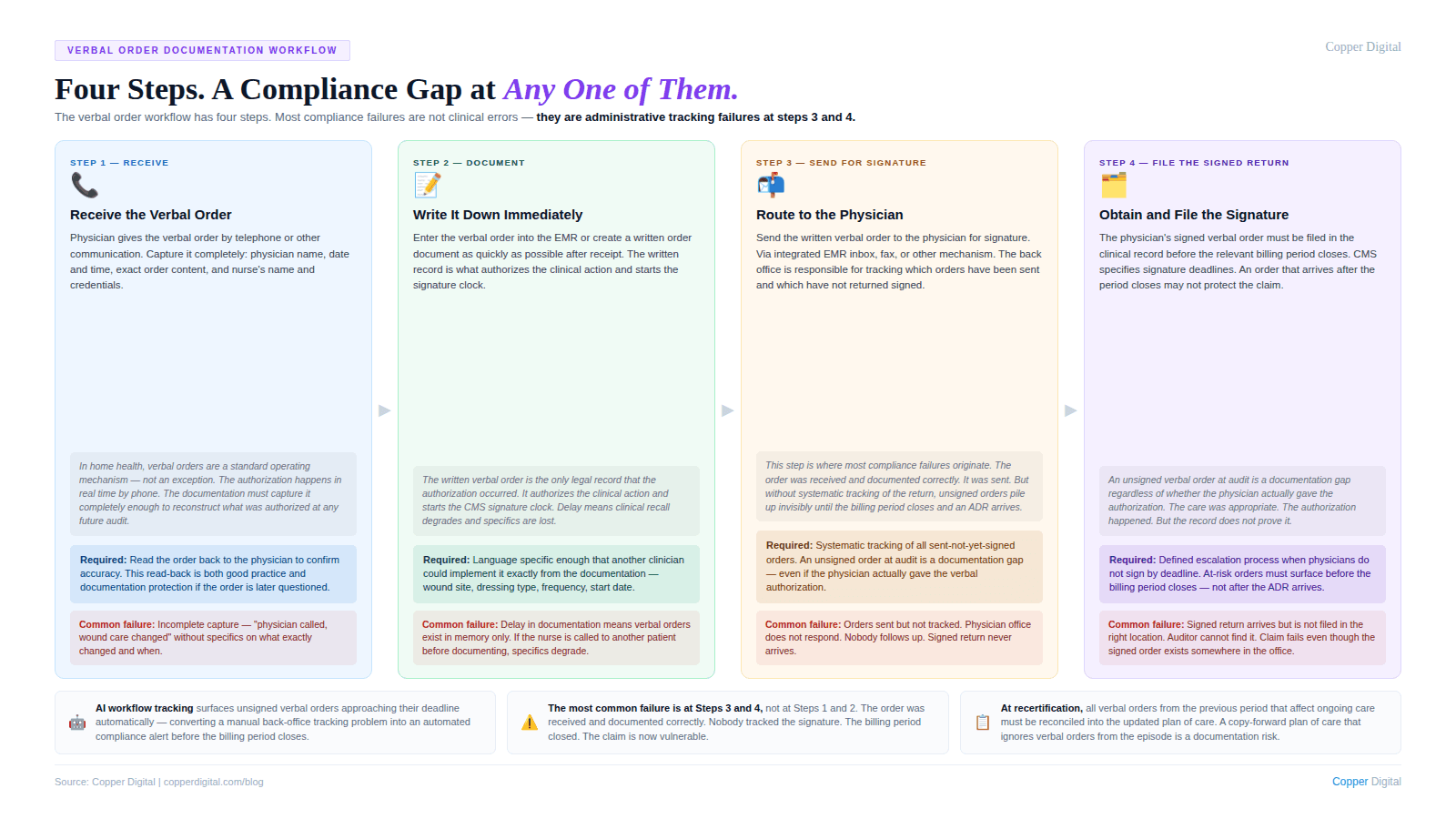
The workflow for verbal orders in home health has four steps. Problems at any step create documentation gaps that affect claim defensibility.
Step 1: Receive the verbal order
When the physician gives a verbal order by telephone or other communication, the nurse receiving the order must capture it accurately and completely. This means recording the physician's name, the date and time of the order, the specific order content, and the nurse's name and credentials. The language for the order should be specific enough that another clinician reading it would know exactly what was authorized.
Verbal orders received over the phone should be read back to the physician to confirm accuracy. This read-back is good clinical practice and also documentation protection: if the order is later questioned, the nurse can confirm that the content was verified with the physician at the time it was given.
Step 2: Document the verbal order in writing immediately
As quickly as possible after receiving the verbal order, the nurse must create a written record of it. In EMR-based agencies, this means entering the order into the EMR as a verbal order. In non-EMR environments, it means creating a written order document. The written documentation should capture everything from Step 1 and should reflect the exact terms of what was authorized.
The written verbal order then becomes part of the clinical record. It authorizes the nurse to proceed with the ordered clinical change. It also starts the clock on getting the physician's signature.
Step 3: Send the written verbal order to the physician for signature
The written verbal order must be sent to the physician for signature. The mechanism for this depends on the agency's workflow and the physician's practice setup. Agencies with integrated EMR systems may be able to route the order directly to the physician's inbox for electronic signature. Agencies without that integration typically fax the order to the physician's office.
The agency's back office is responsible for tracking which verbal orders have been sent and which have not been signed. Unsigned verbal orders require follow-up. This is an administrative tracking function that should be systematized, not left to individual nurses to manage.
Step 4: Obtain and file the physician's signature
The physician's signed verbal order must be filed in the patient's clinical record. CMS specifies signature deadlines for verbal orders: orders that are part of the plan of care or that affect plan of care content must generally be signed before the relevant billing period closes. The specific deadlines vary by order type and by how the order relates to the overall plan of care.
An unsigned verbal order at the time of an ADR review or audit is a documentation problem. The care may have been appropriate and the physician may have actually given the verbal authorization, but without the signed written order in the record, the documentation does not support the claim.
Verbal Orders and the Plan of Care: How They Interact
The plan of care is the formal physician order document that authorizes home health services for the 60-day certification period. Verbal orders are the mechanism for clinical changes that occur within that period. Understanding how they interact is essential for maintaining a coherent clinical record. For a detailed explanation of the relationship between the care plan and the plan of care, see our post on the start of care visit.
Verbal orders within the certification period
During an active certification period, verbal orders authorize individual clinical changes. Each verbal order is signed independently by the physician. The accumulated signed verbal orders, together with the original plan of care, form the complete authorized clinical record for the episode. A chart auditor reviewing the record should be able to trace every clinical action back to either the original plan of care or a subsequent signed verbal order.
Verbal orders at recertification
When the certification period ends and the plan of care is renewed for a new 60-day period, the accumulated verbal orders from the previous period are reconciled into the new plan of care. Any clinical changes that were authorized by verbal order during the previous period and that continue into the new period should be reflected in the updated plan of care at recertification. This is one of the reasons the recertification plan of care should not be a copy-forward of the original: it must reflect the clinical changes that occurred during the episode.
When a verbal order affects the plan of care
If a verbal order makes a change significant enough to materially affect the plan of care, the agency may need to issue a revised plan of care for physician signature, rather than simply filing the verbal order. The threshold for what requires a full plan of care revision versus a standalone verbal order varies by agency policy and by the nature of the change, but the principle is that the physician should have signed documentation of all material aspects of the patient's authorized care plan.
Common Verbal Order Documentation Failures
Unsigned verbal orders at audit
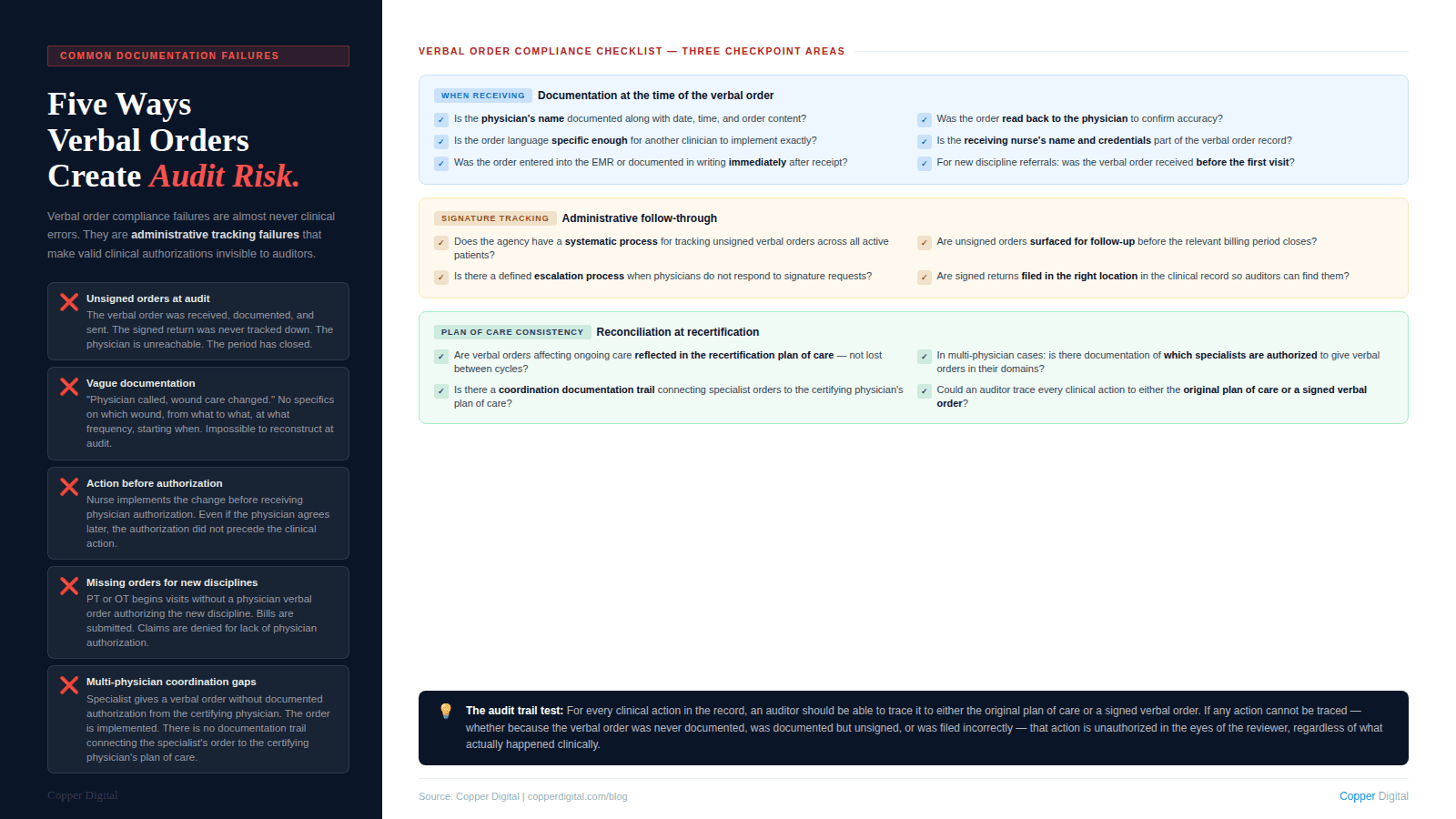
The most common verbal order compliance failure is unsigned orders in the chart at the time of an audit or ADR review. The verbal order was received. It was documented in writing. It was sent to the physician. But the signed return was never tracked down and filed. The back office did not follow up. The physician's office did not respond promptly. The signed order is somewhere in the fax queue or the inbox. This is an administrative process failure, and it shows up in the clinical record as a documentation gap.
Verbal orders documented vaguely
A verbal order documented as "physician called, changes to wound care approved" is not a compliant verbal order record. The order must specify exactly what was changed: which wound, from what dressing to what dressing, at what frequency, starting on what date. Vague verbal order documentation makes it impossible to reconstruct what was actually authorized if the order is questioned later.
Clinical actions taken before a verbal order is received
Occasionally, nurses implement clinical changes before receiving physician authorization, particularly in cases where the clinical need seems obvious and the nurse expects the physician to agree. This is a practice that creates liability. If the physician does not agree, the nurse has performed unauthorized care. If the physician agrees but the verbal order is not documented until after the fact, the record does not support the authorization chain. Clinical changes must be authorized before they are implemented, even when the authorization process is a brief telephone call.
Missing verbal orders for new discipline referrals
A physical therapist begins seeing a patient based on a nurse's clinical recommendation without a signed physician order authorizing the PT evaluation and treatment. The PT bills for services rendered. The claim is denied because there is no physician order authorizing the PT service. This is a specific and preventable failure. Any new discipline addition requires a verbal order from the physician before the service begins. This is the same documentation logic that governs face-to-face documentation requirements: the physician authorization must precede the clinical action, not follow it.
Managing Verbal Orders in Multi-Physician Cases
When a patient has multiple treating physicians, verbal order management becomes more complex. CMS requires that home health services be under the care of one certifying physician who is responsible for the overall plan of care. Other treating physicians may provide care within their specialty, but their verbal orders must be coordinated through the certifying physician's authorization structure.
In practice, this means the nurse must know which physician is authorized to give verbal orders for which aspects of the patient's care. If the cardiologist is managing the cardiac medications and the endocrinologist is managing the diabetes, and the certifying physician has documented that these specialists are authorized to give verbal orders within their domains, then the nurse can receive verbal orders from those specialists within those domains. Without that documented authorization, only the certifying physician's verbal orders are valid.
The documentation requirement is a record of coordination: the nurse should document communications with treating specialists and note the certifying physician's awareness and concurrence with orders from other physicians. This coordination documentation is what protects the claim when an auditor asks why an endocrinologist's verbal order for an insulin dose change is in a record that names a primary care physician as the certifying physician.
How AI-Assisted Workflows Address the Verbal Order Gap
The verbal order compliance failures described above are almost entirely administrative tracking failures, not clinical judgment failures. The nurse received the verbal order correctly. She documented it accurately. She sent it for signature. But the back-end tracking process did not ensure the signed return was filed before the billing period closed.
AI-assisted workflow tools can systematize verbal order tracking in ways that manual administrative processes cannot reliably do at volume. When a verbal order is documented in the EMR, the system can automatically track its signature status, surface unsigned orders that are approaching deadline, and trigger follow-up to the physician's office without requiring a coordinator to manually review every active order across every active patient.
This is the same administrative automation logic that drives scheduling milestone alerts and pre-submission validation checks. Compliance failures that stem from administrative tracking gaps are not clinical problems. They are workflow problems with workflow solutions.
Verbal Order Documentation Checklist
Use this checklist to evaluate your agency's verbal order process against compliance requirements.
When receiving a verbal order
Is the physician's name, the date and time of the order, the specific order content, and the receiving nurse's name and credentials documented?
Was the order read back to the physician to confirm accuracy?
Is the order language specific enough that another clinician could implement it exactly from the written documentation?
Written documentation
Is the verbal order entered into the EMR or documented in writing immediately after receipt?
Does the written documentation include all required elements: who gave the order, when, what exactly was ordered?
Is the written verbal order distinguishable in the record from nursing notes and visit documentation?
Signature tracking
Does the agency have a systematic process for tracking unsigned verbal orders?
Are unsigned orders surfaced for follow-up before the relevant billing period closes?
Is there a defined escalation process when physicians do not respond to verbal order signature requests?
Plan of care consistency
Are verbal orders that affect the plan of care content reflected in the recertification plan of care at the next certification cycle?
Are new discipline referrals authorized by verbal order before the service begins?
In multi-physician cases, is there documentation of which physicians are authorized to give verbal orders within their domains?
Copper Digital's AI workflow tools track verbal order signature status across your active caseload, surface unsigned orders approaching deadline, and trigger follow-up before the billing period closes — converting a manual administrative tracking problem into an automated compliance workflow. Request a demo to see how this works in your agency. |
Related Reading

