Blog
Mar 10, 2026
Why Your Scheduling Process Is Your Biggest Documentation Risk

Arvind Sarin

Most home health agencies treat scheduling as an administrative function. Someone builds a schedule, clinicians follow it, coordinators adjust it when things fall apart. The technology that supports it, if any, is a calendar tool or a basic EMR scheduling module designed to track who goes where.
This framing is wrong, and it costs agencies in ways that never show up on a scheduling report.
Scheduling in home health is a clinical continuity decision. Every assignment choice, which nurse sees which patient, how consistently, with what notice, on what timeline relative to start of care and recertification, determines the quality of the documentation that comes out of that visit. And documentation quality determines reimbursement, audit risk, HHVBP performance scores, and patient outcomes. The scheduling desk and the billing department are not separate functions. They are the same function with a delay between them.
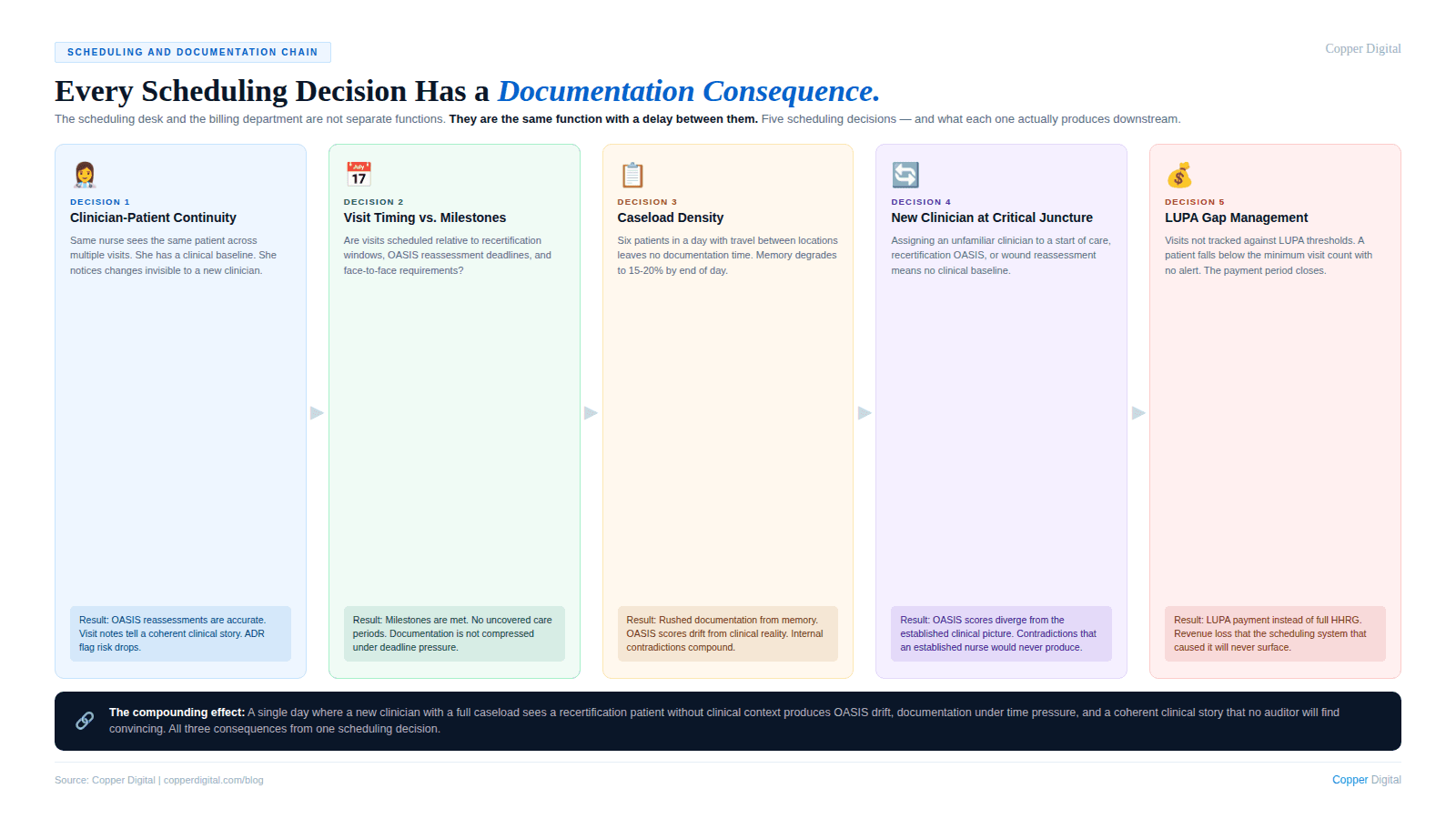
The Scheduling Decisions That Drive Documentation Quality
There are four scheduling decisions that directly determine whether a home health episode produces accurate, defensible documentation or fragmented, inconsistent records.
1. Clinician-patient continuity
When the same nurse sees the same patient across multiple visits, she builds a clinical picture over time. She knows what the patient looked like at start of care. She notices changes in ambulation, cognition, wound status, medication adherence, and home environment that would be invisible to a new clinician starting from scratch.
This continuity matters for documentation in a specific way: the nurse who has context documents differently than the nurse who does not. Her OASIS reassessment scores are more accurate because she has a baseline. Her visit notes tell a coherent clinical story because she is continuing a narrative she knows. The contradictions between OASIS scores and visit note narratives that generate ADR flags are far more likely when a rotating cast of clinicians produces a chart where nobody has complete context.
Agencies that treat scheduling as a pure logistical optimization, minimizing drive time and maximizing visit density, routinely sacrifice continuity in ways that degrade documentation quality across the board. The scheduling decision that saved 20 minutes of drive time cost the agency coherent clinical documentation and increased audit exposure.
2. Visit timing relative to clinical milestones
Home health has defined clinical milestones that carry specific documentation and compliance requirements: start of care, recertification, OASIS reassessment windows, and discharge. The timing of visits relative to these milestones is not flexible. Miss the OASIS reassessment window and you have a compliance problem. Miss the recertification deadline and you have an uncovered care period. Schedule a visit too late in the day before a deadline and you have a documentation-under-pressure problem.
Manual scheduling systems, and even many EMR scheduling modules, do not surface these milestone deadlines proactively. They track scheduled visits. They do not alert coordinators that a particular patient's recertification OASIS window opens in three days and the current scheduled visit falls after the window closes. That connection requires cross-referencing the visit schedule against the clinical calendar, which is a separate system, which no coordinator is reliably doing for every patient every day.
3. Caseload density and documentation time
A nurse with six patients scheduled in a day, each requiring 45 minutes of direct care and travel between locations, has no time to document during the day. She is documenting from memory at the end of the day or after dinner. Studies show clinical recall degrades to roughly 15 to 20 percent of specific details by eight hours after a visit. The scheduling decision that packed her day with six patients did not just affect her wellbeing. It affected the accuracy of the OASIS assessments and visit notes for all six of those patients. This is the documentation timing problem described in detail in An Autopsy of a Start of Care.
Caseload density is a scheduling decision. Agencies that schedule for maximum utilization without accounting for documentation time are making a choice to accept degraded documentation quality. The LUPA risk, the audit risk, and the HHVBP score impact are downstream consequences of that choice, and they are invisible in the scheduling system that made it.
4. New clinician assignments at critical junctures
Assigning an unfamiliar clinician to a patient at a high-stakes clinical moment, a start of care, a recertification OASIS, a wound reassessment, creates compounded documentation risk. The clinician has no clinical baseline for this patient. She is working cold from whatever she can pull from the chart, which may itself be incomplete. Her OASIS scores may diverge from the established clinical picture in ways that create internal inconsistencies the prior clinician would never have produced.
Scheduling systems that treat all visit slots as interchangeable, assigning whoever is available regardless of clinical context, produce this pattern routinely. It is not a clinical failure. It is a scheduling failure with clinical consequences.
The scheduling desk and the billing department are not separate functions. They are the same function with a delay between them. Every bad scheduling decision shows up in the documentation, and every documentation problem shows up in the revenue. |
The LUPA Problem Is a Scheduling Problem
Low Utilization Payment Adjustments are one of the most direct financial consequences of scheduling failures in home health. Under PDGM, a 30-day payment period that falls below the minimum visit threshold receives a reduced payment that may not cover the cost of the care delivered. LUPAs happen for two reasons: patients refuse visits, or visits are not scheduled and delivered.
The second category, visits not scheduled and delivered, is a scheduling failure. It happens when coordinators lose track of visit frequency requirements across a growing caseload, when scheduling gaps open up around weekends or holidays and are not filled, when a patient is deprioritized because their case seems stable, or when a clinician calls out and the replacement visit is never scheduled.
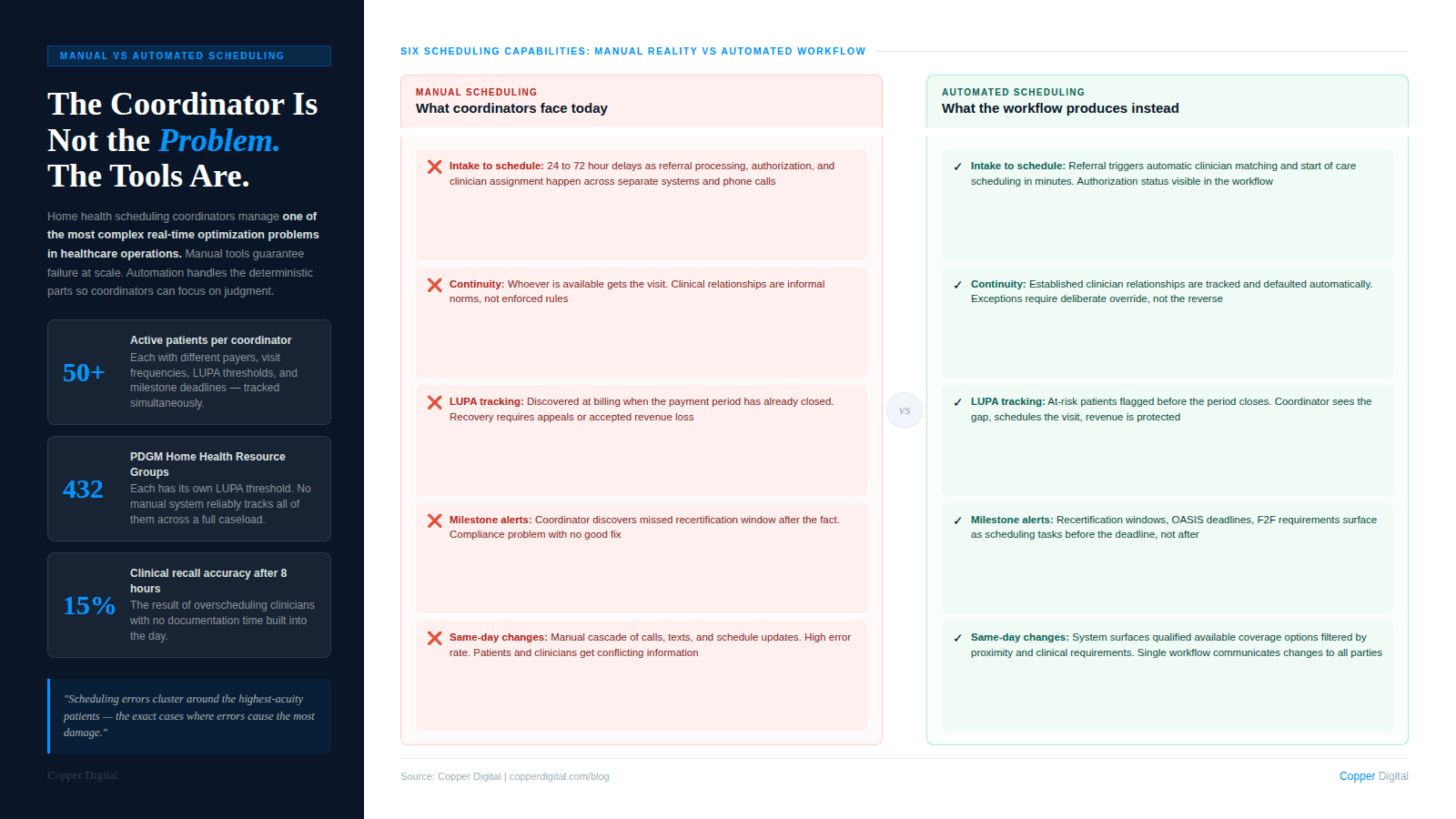
Manual scheduling at any meaningful volume cannot reliably prevent LUPAs. The coordinator managing 50 active patients across multiple clinicians and multiple payers, tracking visit frequency requirements for each, identifying patients approaching the LUPA threshold and ensuring coverage, is doing a calculation that is too complex to do accurately by hand. Agencies that accept LUPA rates as a normal cost of doing business are accepting a preventable revenue loss as a feature of their scheduling process.
LUPA thresholds under PDGM Under PDGM, each of the 432 Home Health Resource Groups has a defined LUPA threshold, the minimum number of visits required within a 30-day payment period to receive the full HHRG payment. The threshold varies by clinical grouping. Agencies managing high volumes of patients across multiple clinical groupings cannot track all of these thresholds manually with any reliability. Automated scheduling tools that flag patients approaching their LUPA threshold before the period closes convert this from a reactive revenue recovery problem into a preventable scheduling decision. |
The Hidden Cost of Manual Scheduling: Coordinator Time and Error Rate
Home health scheduling coordinators are among the most cognitively burdened staff in any agency. They are managing availability across a clinician roster, balancing geographic efficiency with clinical continuity, tracking visit frequency requirements and clinical milestones, responding to same-day changes when clinicians call out, managing patient availability and preferences, and communicating schedule changes to clinicians, patients, and families.
All of this is happening in real time, across a system that is typically a combination of an EMR scheduling module, a spreadsheet, a whiteboard, and phone calls. The error rate in this environment is not a reflection of the coordinator's competence. It is a structural consequence of the complexity of the task and the inadequacy of the tools.
The errors that result are not random. They cluster around the most complex cases, the highest-acuity patients who need the most precise scheduling, and around high-volume periods, the times when scheduling errors are most likely to cause the most damage. A new admission on a Friday afternoon, a recertification patient whose OASIS window opens over a holiday weekend, a high-acuity patient assigned to a new clinician because the regular nurse is out, these are the cases where manual scheduling fails most visibly and most consequentially.
What coordinator time actually costs
The scheduling coordinator's time has an opportunity cost that agencies rarely account for. Every hour spent on manual scheduling adjustments, gap-filling, and communication is an hour not spent on prior authorization follow-up, referral source relationship management, or clinical quality review. The scheduling function is not just a cost center; it is a constraint on every other administrative function the agency needs to perform.
Agencies that have automated significant portions of their scheduling workflow report that coordinators shift from reactive crisis management to proactive capacity planning. The work does not disappear. It changes from firefighting to oversight, which is a fundamentally different and more productive use of skilled administrative staff.
What Scheduling Automation Actually Addresses
Scheduling automation in home health is not about replacing coordinators with algorithms. It is about handling the deterministic, rule-based portions of scheduling reliably so that coordinators can focus on the judgment-intensive portions.
Intake-to-schedule automation
When a referral arrives, the scheduling workflow begins immediately: confirm insurance authorization, verify the patient's availability and location, identify the right clinician based on proximity, specialization, and patient history, and schedule the start of care visit within the timeframe required by payer and regulatory requirements.
Manual intake-to-schedule processes at agencies receiving high referral volumes routinely delay start of care visits by 24 to 72 hours. Those delays have clinical consequences (care that was supposed to begin does not), documentation consequences (the start of care OASIS and visit note are compressed under time pressure), and revenue consequences (a delayed start of care is a delayed billing clock). Automated intake workflows that move from referral receipt to scheduled start of care visit in minutes rather than hours address all three consequences simultaneously. This connects directly to the referral processing gaps that affect PDGM coding accuracy at the very start of the episode.
Continuity-first assignment logic
Automated scheduling tools can enforce continuity rules that manual systems cannot maintain at scale. If a patient has an established clinician relationship, the system defaults to that clinician unless a specific exception applies. If a visit requires clinical specialization (wound care, cardiac management, post-surgical rehab), the system filters candidates accordingly. If a patient is approaching a recertification OASIS, the system prioritizes the clinician with the most visit history for that patient.
These rules exist in most agencies as informal norms that coordinators try to apply when they have time. Automated enforcement makes them systematic rather than aspirational.
LUPA threshold monitoring
An automated scheduling system that tracks visit counts against LUPA thresholds by patient and payment period surfaces at-risk patients before the period closes. The coordinator sees a dashboard showing which patients are below their threshold, how many visits remain in the period, and what the scheduling options are to fill the gap. This converts LUPA prevention from a reactive billing recovery task into a proactive scheduling decision.
Clinical milestone alerts
Recertification windows, OASIS reassessment requirements, face-to-face documentation deadlines, and discharge planning milestones can all be surfaced as scheduling alerts. A coordinator who sees that Patient A's recertification OASIS window opens in four days and no visit is currently scheduled in that window can act before the window closes. A coordinator who discovers this on day 61 cannot.
Same-day change management
When a clinician calls out, the cascade of scheduling changes required to cover their patients is the most disruptive and error-prone part of the coordinator's day. Automated change management tools that identify coverage options, filter by geographic proximity and clinical qualifications, and communicate changes to patients and clinicians in a single workflow reduce the cognitive load and error rate of this process significantly.
The Documentation Quality Connection
Every scheduling improvement that increases clinician-patient continuity, reduces caseload pressure, and ensures visits happen on clinically appropriate timelines has a direct effect on documentation quality.
A nurse who sees the same patient consistently documents more accurately because she has context. A nurse whose caseload is appropriately sized documents more accurately because she has time. A nurse who arrives at a visit with a pre-visit briefing generated from the patient's prior documentation documents more accurately because she is not starting from a cold chart. These are not separate initiatives. They are the same initiative: building a scheduling and documentation workflow where the clinical information available at each visit supports accurate, complete, timely documentation rather than working against it. The pre-visit briefing component of this is covered in detail in Your EMR Was Not Built for Your Nurses.
The agencies that are performing best on HHVBP quality measures, achieving the lowest ADR denial rates, and maintaining the highest OASIS accuracy scores are not doing so because they hired better nurses. They are doing so because their operational workflows, including their scheduling workflows, are structured to support clinical accuracy rather than to undermine it.
A scheduling system that maximizes utilization without accounting for documentation time, clinical continuity, or milestone deadlines is not optimizing agency performance. It is trading short-term productivity for long-term revenue and compliance risk. |
A Scheduling Automation Readiness Checklist
Use this checklist to evaluate where your current scheduling process creates the most documentation and revenue risk.
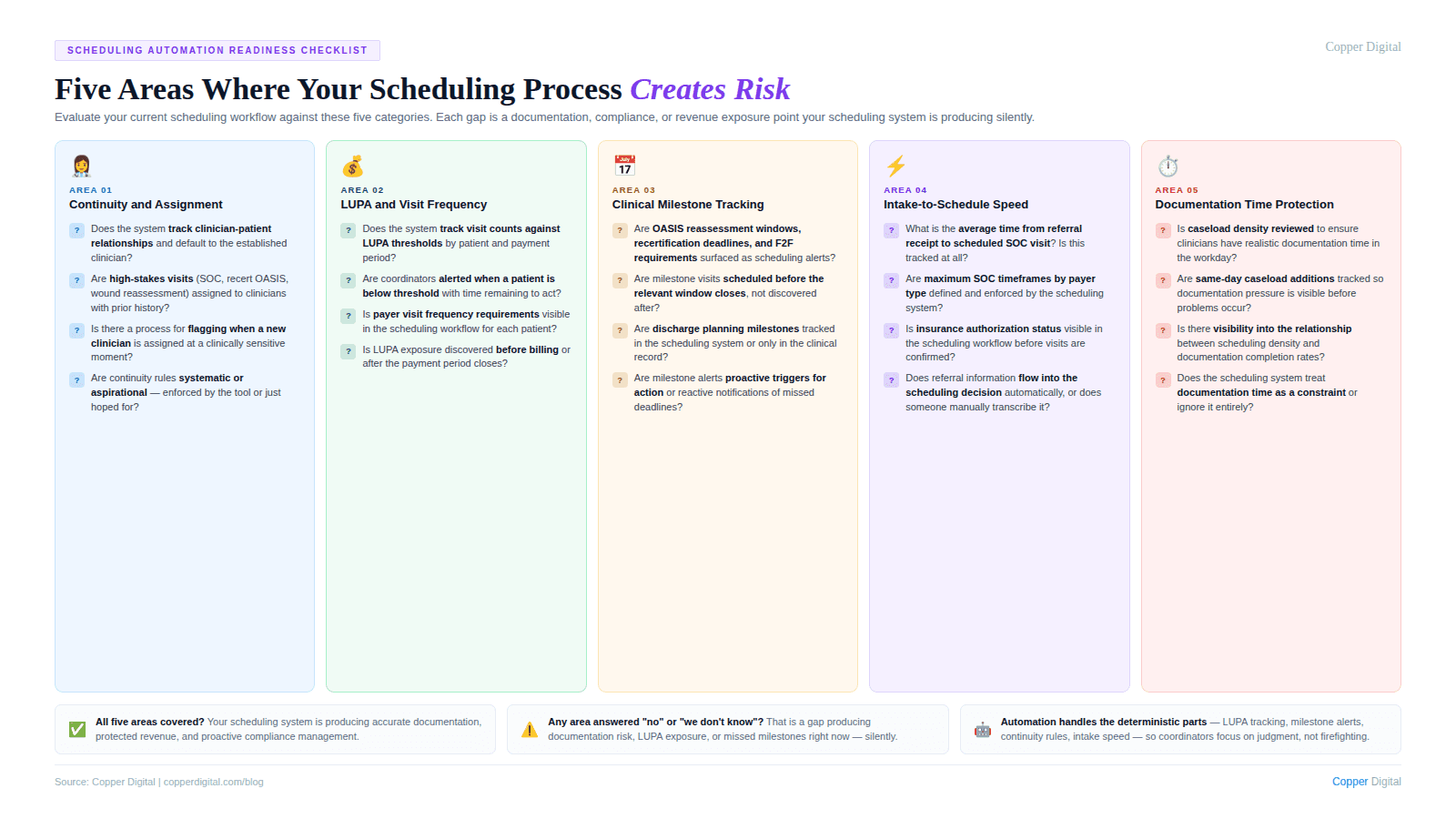
Continuity and assignment
Does the scheduling system track clinician-patient relationships and default to the established clinician when available?
Are high-stakes visits (start of care, recertification OASIS, wound reassessment) assigned to clinicians with prior visit history for that patient when possible?
Is there a process for identifying when a new clinician is being assigned to a patient at a clinically sensitive moment?
LUPA and visit frequency
Does the scheduling system track visit counts against LUPA thresholds by patient and payment period?
Are coordinators alerted when a patient is below their threshold with time remaining to schedule additional visits?
Is there visibility into which payer visit frequency requirements apply to each patient?
Clinical milestone tracking
Are OASIS reassessment windows, recertification deadlines, and face-to-face documentation requirements surfaced as scheduling alerts?
Is there a system for ensuring that clinical milestone visits are scheduled before the relevant window closes?
Are discharge planning milestones tracked in the scheduling system or only in the clinical record?
Intake-to-schedule efficiency
What is the average time from referral receipt to scheduled start of care visit? Is this measured?
Are there defined maximum timeframes for different payer types, and is the scheduling system enforcing them?
Is insurance authorization status visible in the scheduling workflow before visits are confirmed?
Documentation time protection
Is caseload density reviewed to ensure clinicians have realistic documentation time within the workday?
Are same-day caseload additions tracked to understand when documentation pressure is highest?
Is there visibility into the relationship between scheduling density and documentation completion rates?
What to Look for in a Home Health Scheduling Automation Tool
Not all scheduling automation tools are built for home health's specific operational requirements. When evaluating options, the capabilities that matter most are:
Clinical continuity logic. The tool should track clinician-patient relationships and apply continuity preferences automatically, not just as a manual flag a coordinator can optionally apply.
PDGM-aware visit tracking. The tool should understand LUPA thresholds by HHRG grouping and surface at-risk patients before the payment period closes, not just after billing.
Milestone-based scheduling alerts. Recertification windows, OASIS reassessment requirements, and face-to-face deadlines should trigger scheduling alerts proactively, not reactively.
Referral-to-schedule integration. The scheduling workflow should begin at referral receipt, not after intake is manually completed. Authorization status, patient demographics, and care requirements should flow from the referral into the scheduling decision.
Real-time caseload visibility. Coordinators should see clinician caseloads, geographic distribution, and documentation burden in real time, not in a report generated the next morning.
Same-day change management. When a clinician is unavailable, the tool should surface qualified, available coverage options filtered by clinical requirements and geography, and communicate changes to all parties in a single workflow.
Copper Digital's scheduling automation connects referral intake, clinician assignment, LUPA monitoring, and clinical milestone tracking in a single workflow designed specifically for home health operations. Request a demo to see how scheduling automation changes the documentation and revenue picture for your agency. |
Related Reading
Why Home Health Agencies Fail ADR and TPE Audits: It Is Not the Care. It Is the Documentation.
An Autopsy of a Start of Care: The 2-Hour Visit That Takes 6 Hours
Home Health Recertification Documentation: Why Renewal Is Not Enough and What CMS Actually Requires
Your EMR Was Not Built for Your Nurses: Kathy Duckett Explains Why

