Blog
Mar 6, 2026
Home Health Recertification Documentation: Why Renewal Is Not Enough and What CMS Requires

Arvind Sarin
The second 30-day payment period begins. The clinical supervisor approves the recertification. The physician signs the updated plan of care. The OASIS is completed. And somewhere in that workflow, the documentation that actually justifies why this patient still needs home health services, that specific, clinical, evidence-based justification, never gets written.
Recertification is one of the most consistently audited events in home health and one of the most consistently underdocumented. Agencies treat it as an administrative renewal when CMS requires it to be a fresh clinical argument. This post explains exactly what that argument must contain, why it fails so often, and what has to change to make recertification documentation audit-ready before the ADR arrives.
What Recertification Actually Is and What It Is Not
A home health episode under Medicare consists of 60-day certification periods. Within each 60-day period, there are two 30-day payment periods under PDGM. When a patient continues to require home health services beyond the initial certification period, the agency must recertify, obtain a new physician certification that the patient continues to meet home health eligibility criteria.
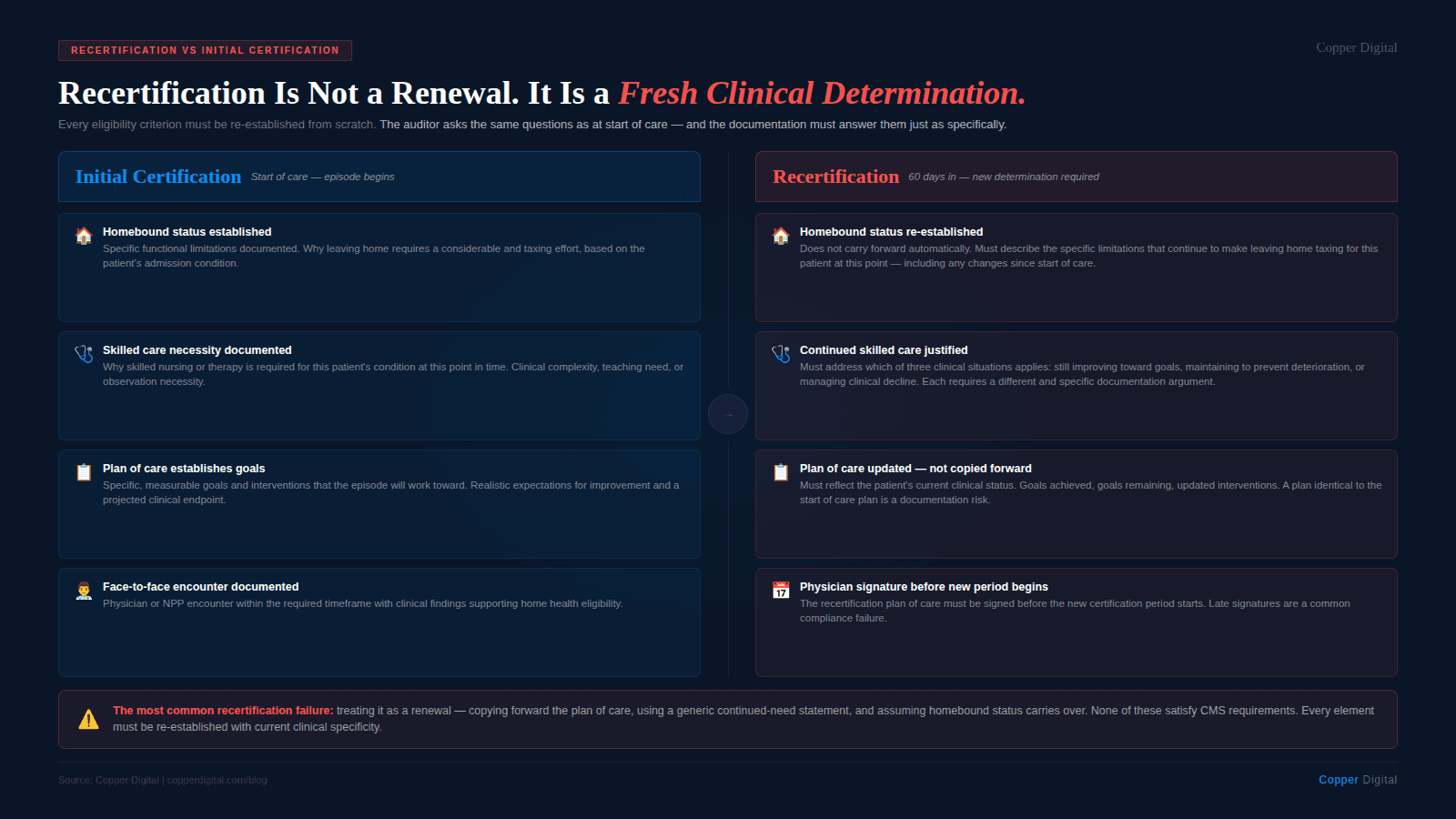
The word renewal is the problem. Recertification is not a renewal. It is not an extension. It is a new clinical determination that the patient, at this point in time, still meets the eligibility criteria for Medicare home health services. That means homebound status must be re-established, skilled care necessity must be re-justified, and the plan of care must reflect the current clinical picture rather than carrying forward goals and interventions from the original episode.
An auditor reviewing a recertification period is asking the same questions they ask at start of care: Is this patient homebound? Does this patient require skilled care? Is the care being delivered medically necessary? The only difference is that the baseline is now different. The patient has received care for 60 days. If they have improved, the documentation must explain why continued skilled care is still necessary. If they have not improved, the documentation must explain why continued skilled care is clinically reasonable despite lack of progress.
Recertification is not a renewal. It is a fresh clinical determination that this patient, today, still meets every eligibility criterion for Medicare home health. The documentation must make that case from scratch — not assume it carries over from the original certification. |
The Four Elements CMS Requires at Recertification
For a recertification to be valid and defensible under audit, four elements must be present and documented:
1. Continued homebound status
Homebound status does not carry forward automatically. The recertification documentation must establish that the patient, at the time of recertification, still meets the homebound definition: leaving home requires a considerable and taxing effort due to the patient's condition. The same specificity requirements that apply at start of care apply at recertification. A note that says patient remains homebound is not sufficient. The documentation must describe the specific functional limitations that continue to make leaving home taxing for this patient at this point in the episode.
2. Continued skilled care necessity
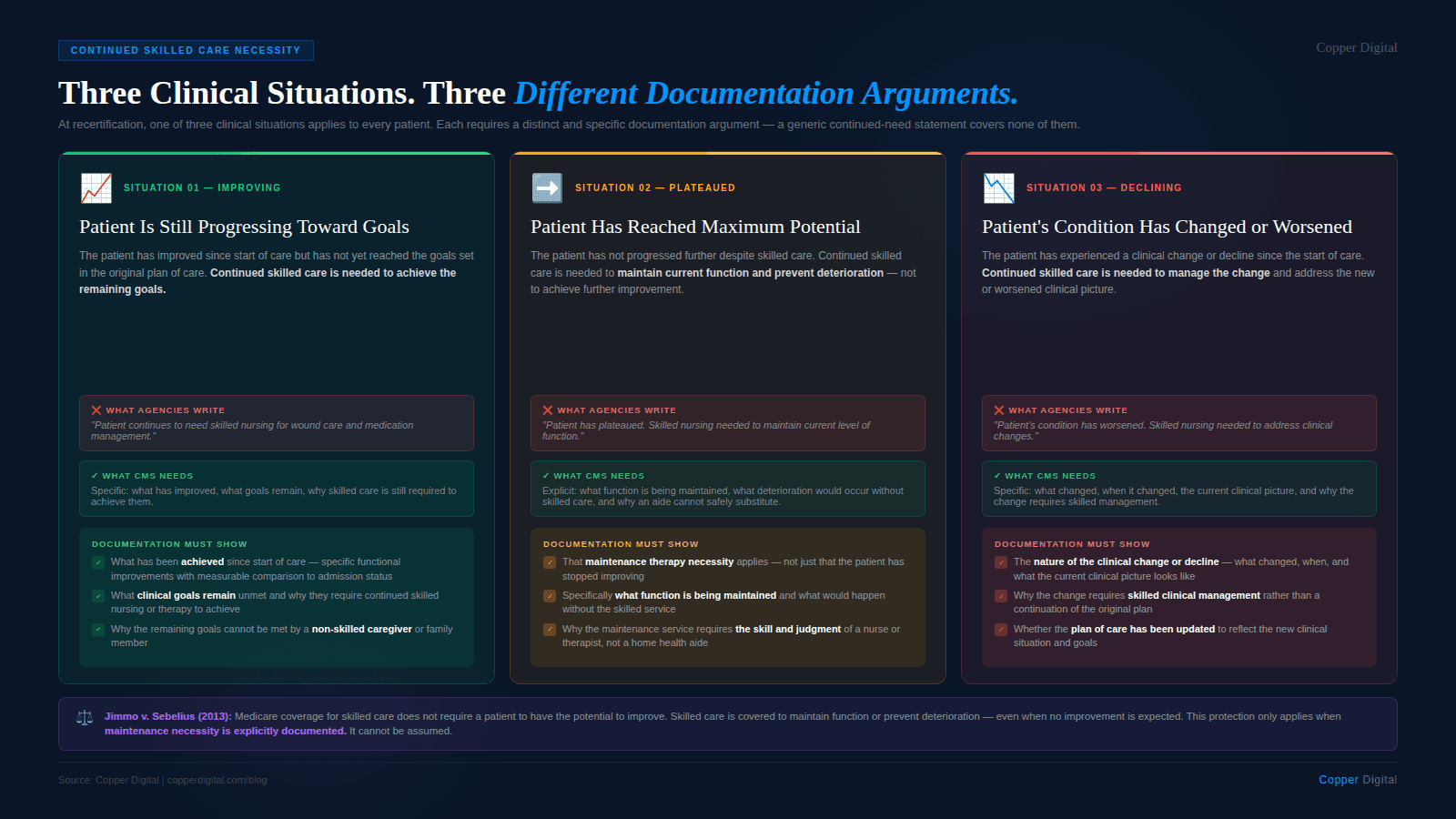
The recertification must justify why skilled nursing or therapy services are still required. This is where most recertification documentation fails. The original episode justified skilled care based on the patient's condition at admission. By the recertification point, one of three clinical situations applies:
The patient has improved and continued skilled care is needed to progress toward remaining goals. The documentation must describe what has improved, what clinical goals remain unmet, and why continued skilled nursing or therapy is required to achieve them.
The patient has plateaued and maintenance therapy or skilled oversight is medically necessary to prevent deterioration. The documentation must establish maintenance necessity explicitly, not just note that the patient is not progressing.
The patient has declined and continued skilled care is needed to address the clinical change. The documentation must describe the nature of the decline and why skilled care is required to manage it.
Each of these situations requires specific documentation. A recertification note that says patient continues to need skilled nursing without specifying which of these three clinical situations applies, and why, is vulnerable to denial.
3. A recertification OASIS that reflects the current clinical picture
The recertification OASIS — the SOC OASIS, Follow-Up OASIS, or Recertification OASIS depending on episode timing — must accurately reflect the patient's functional status at the time of recertification, not carry forward scores from the start of care. The same accuracy requirements that apply at start of care apply at recertification. Internal inconsistencies between OASIS scores and clinical narrative are as damaging at recertification as they are at initial certification — and they raise additional questions about whether the clinical picture at recertification is being accurately represented.
4. A physician-signed plan of care that reflects current goals and interventions
The recertification plan of care must be signed by the certifying physician before the new certification period begins. It must reflect the patient's current condition and goals — not be a copy-forward of the original plan of care with updated dates. If the patient's goals have changed because they have achieved some and not others, the plan of care must reflect that. If the clinical focus has shifted, the plan of care must reflect that. A plan of care that is identical to the initial certification except for the dates is a documentation risk.
The Three Recertification Documentation Failures That Drive Denials
Failure 1: The continued-need statement is generic
The most common recertification documentation failure is a continued-need statement that could apply to any patient at any point in any episode: patient continues to require skilled nursing for wound care and medication management. This tells an auditor nothing about why this patient still needs skilled care at this point in the episode. It does not describe what has happened clinically since the start of care. It does not establish why the goals have not yet been met or why continued skilled intervention is necessary. It is a placeholder, not a clinical justification.
Failure 2: The plan of care is a copy-forward
A recertification plan of care that is substantively identical to the start of care plan — same goals, same interventions, same visit frequency — without clinical narrative explaining why the same approach is still appropriate sends a specific audit signal: this agency is not actively managing this patient toward discharge. CMS expects that goals will evolve over the course of a home health episode. A plan of care that has not changed after 60 days of care either reflects excellent clinical documentation that explains why no adjustment was needed, or it reflects a failure to actively reassess and document the patient's clinical trajectory.
Failure 3: Maintenance necessity is implied rather than documented
For patients who have reached maximum functional potential but require ongoing skilled care to prevent deterioration — the maintenance therapy population — the clinical justification at recertification is specific and distinct from the restorative justification that applied at start of care. Maintenance necessity must be explicitly documented. The documentation must establish that the patient's condition requires the skill, knowledge, and judgment of a skilled therapist or nurse to maintain function, and that without the skilled service, the patient would deteriorate in ways that are clinically predictable and documentable.
This is a nuanced clinical argument. The documentation that supports it needs to be specific about what function is being maintained, what would happen without the skilled service, and why a non-skilled caregiver could not safely provide the service. Agencies that do not train their clinicians to document maintenance necessity explicitly will consistently produce recertification documentation that cannot defend ongoing skilled care for patients who genuinely need it.
The Jimmo v. Sebelius standard The 2013 Jimmo v. Sebelius settlement clarified that Medicare coverage for skilled care does not require a patient to have the potential to improve. Skilled care is covered when it is necessary to maintain a patient's current condition or to prevent or slow deterioration, even if no improvement is expected. This is an important protection for agencies serving patients with chronic or degenerative conditions — but it only applies if the maintenance necessity is explicitly documented. Agencies cannot rely on the Jimmo standard to protect claims that do not contain the specific documentation of maintenance necessity that CMS requires. |
The Discharge Planning Problem Hidden Inside Recertification
There is a documentation problem at recertification that agencies rarely name directly: the plan of care never establishes when home health services will end.
Medicare home health was designed as a short-term, episodic benefit. The expectation at start of care is that the agency will define a realistic endpoint — when the patient is expected to achieve independence or maximum function — and orient the clinical work toward that endpoint. At recertification, the documentation must explain why that endpoint has not yet been reached and what the revised clinical trajectory looks like. An agency that recertifies patients repeatedly without ever documenting a projected discharge point is producing a billing pattern that draws audit attention, and the individual clinical records often reflect the same problem: no clinical story that moves toward a defined conclusion.
This does not mean agencies should discharge patients prematurely. It means the clinical documentation at every recertification should reflect active clinical thinking about the episode trajectory — where the patient is, what remains to be achieved, how long that is expected to take, and what the discharge criteria look like.
The clinical documentation at every recertification should reflect active thinking about the episode trajectory — where the patient is, what remains, how long that will take, and what discharge looks like. A recertification that cannot answer those questions is a clinical documentation problem, not just a compliance problem. |
What Compliant Recertification Documentation Looks Like
A compliant recertification does not need to be long. It needs to contain specific clinical content that answers three questions:
Why does this patient still meet homebound criteria? Describe the specific functional limitations that continue to make leaving home a considerable and taxing effort. Reference any changes since the start of care that are clinically relevant to homebound determination.
Why does this patient still require skilled care? Describe the patient's current clinical status, what has been achieved since the start of care, what clinical goals remain, and why achieving them requires skilled nursing or therapy rather than a non-skilled caregiver or family member.
What is the plan for this certification period? Describe the specific goals, interventions, and visit plan for the new certification period, and how they differ from or continue the previous period's plan based on the patient's current clinical status.
For maintenance patients, add: why is skilled care necessary to maintain this patient's current function, what would happen without it, and why a non-skilled caregiver cannot safely provide the service.
How AI-Assisted Documentation Addresses the Recertification Gap
Recertification documentation fails for the same reasons start of care documentation fails: the clinician completing the OASIS and writing the recertification note is working from a fragmented picture of what happened during the previous certification period. The visit notes are there, but synthesizing them into a coherent clinical narrative that demonstrates progress, justifies continued need, and establishes a forward-looking plan requires active clinical work that time pressure makes difficult.
Clinical trajectory synthesis
An AI-assisted clinical workflow can synthesize the visit notes from the previous certification period into a structured clinical summary — what was the patient's functional status at start, what interventions were delivered, what changed, and where the patient is now. This gives the clinician completing the recertification the clinical context they need to write a specific continued-need justification rather than a generic one. The information exists in the record. The problem is getting it out of 30 days of individual visit notes and into a usable format before the recertification assessment.
Recertification content validation
Before a recertification is submitted, an AI content check can review the documentation against the required elements — is there a continued homebound justification, is there a specific continued-need statement, does the plan of care reflect the current clinical picture, is the OASIS assessment internally consistent with the clinical narrative. The same pre-submission validation logic that catches start-of-care documentation gaps applies at recertification with the additional check for whether maintenance necessity has been addressed for patients who have reached maximum functional potential.
Discharge trajectory tracking
An AI-assisted platform that tracks progress toward plan of care goals over time surfaces the data that makes recertification documentation specific and defensible: what goals have been met, which remain, what the clinical trajectory looks like, and whether the current visit frequency and intervention plan are aligned with the remaining clinical needs. This makes the recertification a clinical planning event rather than a paperwork event — and the documentation it produces reflects that distinction.
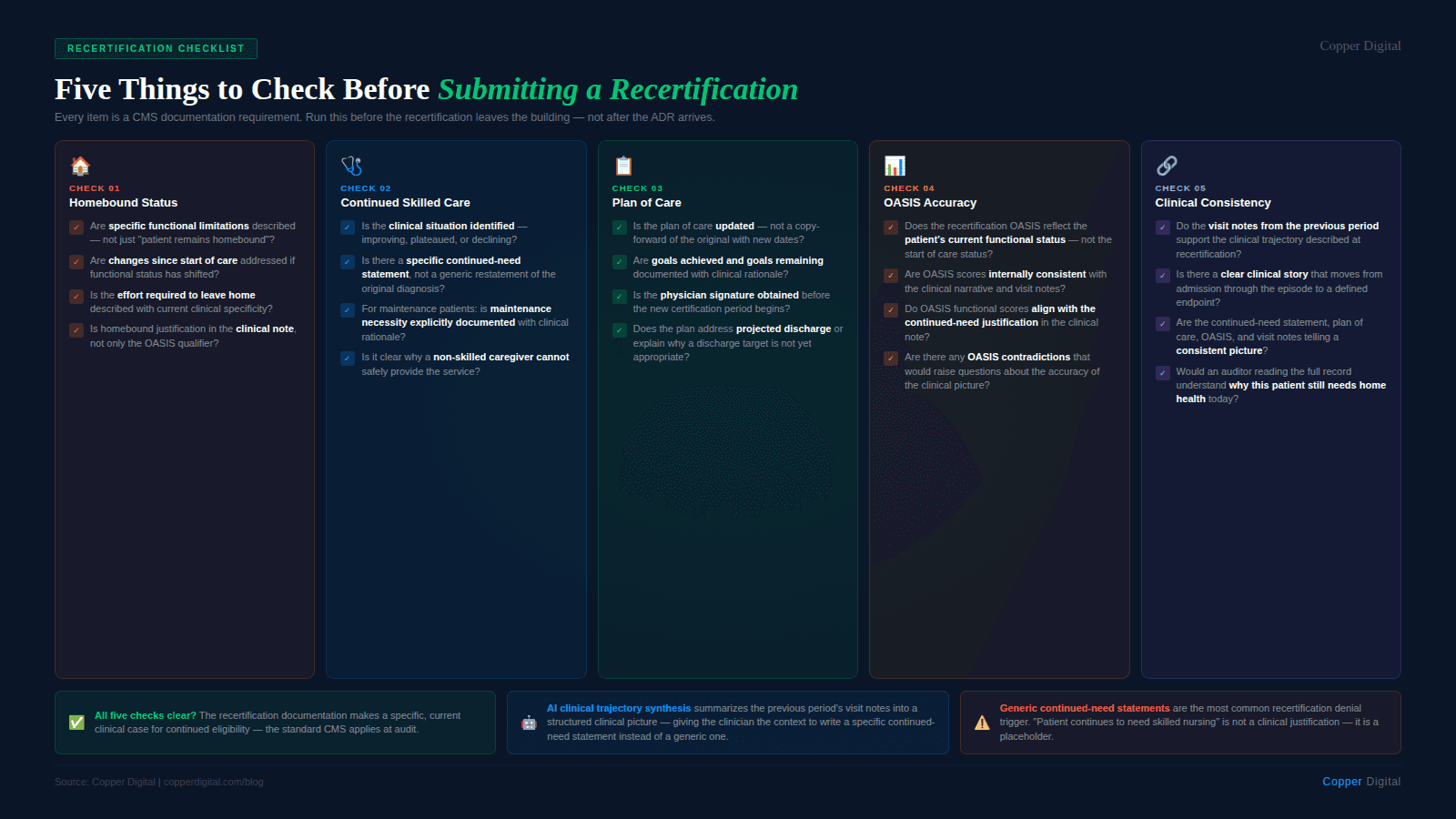
Recertification Documentation Checklist
Use this checklist before submitting a recertification to verify the documentation meets CMS requirements.
Homebound status
Does the documentation re-establish homebound status with specific functional limitations, not just assert that the patient remains homebound?
Are the current limitations described, including any changes since the start of care?
Continued skilled care necessity
Does the documentation describe the patient's current clinical status — what has changed, what has been achieved, what remains?
Is the clinical situation clearly one of: continued restorative need, maintenance necessity, or management of decline — and is that situation specifically documented?
For maintenance patients: is maintenance necessity explicitly documented with specific clinical rationale for why skilled care is required and what would happen without it?
Does the documentation explain why skilled nursing or therapy is required rather than a non-skilled caregiver?
Plan of care
Is the recertification plan of care signed by the certifying physician before the new certification period begins?
Does the plan of care reflect the patient's current clinical status and goals — not a copy-forward of the original plan?
Are updated goals, interventions, and visit frequency documented with clinical rationale?
Does the plan address projected discharge or explain why a discharge target is not yet appropriate?
OASIS accuracy
Does the recertification OASIS reflect the patient's current functional status, not the start of care status? Are scores internally consistent with the clinical narrative? See OASIS accuracy requirements.
Consistency
Is the overall recertification documentation — continued-need statement, plan of care, OASIS assessment, and visit notes from the previous period — telling a consistent clinical story that moves toward a defined clinical conclusion?
Are there any contradictions between the recertification documentation and the visit notes from the previous period that would raise questions about the accuracy of the clinical picture?
Copper Digital synthesizes visit note data from the previous certification period into a structured clinical summary at recertification time, validates continued-need documentation against CMS requirements before submission, and tracks goal progress to make recertification a clinical event rather than a paperwork one. Request a demo to see how this works in your agency's workflow. |
Related Reading

