Blog
Feb 5, 2026
How OASIS Accuracy Drives Your HHVBP Total Performance Score

Arvind Sarin

Your Medicare reimbursement is no longer fixed. Under the Home Health Value-Based Purchasing model, CMS adjusts your payment based on how well your patients do, how often they end up in the hospital, and what they say about their experience. The adjustment runs from negative five percent to positive five percent of your total Medicare fee-for-service revenue.
On a five-million-dollar Medicare book of business, that is a $500,000 swing. And the single largest driver of that swing is your OASIS documentation.
This post breaks down exactly how the HHVBP Total Performance Score is calculated, which OASIS items move it, and what agencies with strong scores are doing differently.
HHVBP is now national. Every Medicare-certified home health agency in the country is scored and paid accordingly. There is no opt-out.
What Is the HHVBP Total Performance Score?
The Total Performance Score, or TPS, is the composite number CMS uses to determine your payment adjustment. It is calculated from three categories of quality measures. You can review the full program details on the CMS HHVBP model page.

1. OASIS-Based Measures
These measures are calculated directly from the OASIS data your clinicians submit. The primary OASIS-based measure driving payment in 2025 is the Discharge Function Score, built from the GG items rather than the older M1800 series. CMS compares the patient's actual discharge GG scores against a risk-adjusted expected score calculated from the Start of Care assessment. You can review the full list of measures on the CMS Home Health Quality Reporting page.
If your clinician underscores functional ability at Start of Care, the expected discharge score is set too low. The patient improves to their actual baseline, and your Discharge Function Score looks worse than the care actually was. You lose credit for outcomes you earned.
2. Claims-Based Measures
These measures are calculated from Medicare claims data. The two primary measures in 2025 are:
Home Health Within-Stay Potentially Preventable Hospitalization (PPH): tracks hospitalizations during the episode that could have been prevented with better management of chronic conditions, infections, or other acute events.
Discharge to Community Post-Acute Care (DTC-PAC): tracks whether patients are successfully discharged to the community rather than to a facility or inpatient setting.
These measures are affected indirectly by OASIS documentation. Accurate clinical staging at Start of Care leads to better care planning, which reduces preventable hospitalizations. Accurate discharge OASIS scoring ensures the DTC-PAC measure captures the real outcome.
3. HHCAHPS Survey-Based Measures
These measures come from the patient experience survey administered after discharge. Patients are asked about communication, care coordination, medication education, and whether they would recommend the agency.
HHCAHPS scores are not directly driven by OASIS, but they are driven by the same clinical conversations that good documentation reflects. Agencies that document patient education thoroughly tend to deliver it more consistently, which shows up in survey results.
The OASIS Items That Move Your TPS
Not all OASIS items are equal in their impact on the TPS. The items with the highest direct influence are the GG functional items, which now drive the Discharge Function Score. You can access the full OASIS data sets and instruments on CMS.gov.
The GG Items: Self-Care and Mobility
The Discharge Function Score is built from a specific set of GG items assessed at both Start of Care and discharge. These include:
GG Item | What It Measures | Timeframe |
|---|---|---|
GG0130A | Eating | SOC and Discharge |
GG0130B | Oral hygiene | SOC and Discharge |
GG0130C | Toileting hygiene | SOC and Discharge |
GG0170A | Roll left and right | SOC and Discharge |
GG0170B | Sit to lying | SOC and Discharge |
GG0170C | Lying to sitting on the side of the bed | SOC and Discharge |
GG0170D | Sit to stand | SOC and Discharge |
GG0170E | Chair/bed-to-chair transfer | SOC and Discharge |
GG0170F | Toilet transfer | SOC and Discharge |
GG0170I | Walking 10 feet | SOC and Discharge |
GG0170J | Walking 50 feet with two turns | SOC and Discharge |
GG0170R | Picking up an object | SOC and Discharge |
Each item is scored on a scale of 1 to 6, where 1 is dependent and 6 is independent. The scoring asks what the patient actually does, not what they could do if they tried. Clinicians who score based on point-in-time observation rather than the patient's typical function introduce inaccuracy that compounds across the episode.
CMS risk-adjusts the expected discharge score based on the Start of Care assessment. An underscored SOC creates an artificially low bar. A clinician who scores a patient as more impaired than they actually are may inadvertently make the agency look like it failed to improve the patient.
The M1800 Series: Still Relevant for Care Planning
The M1800 series, covering grooming, dressing, bathing, toileting, transferring, and ambulation, is no longer the primary driver of the Discharge Function Score. However, these items still feed into OASIS-based quality measures on Home Health Compare and remain important for care planning, QA consistency, and audit defensibility.
Inconsistencies between M1800 items and GG items within the same OASIS are a red flag in QA review and payer audits.
Process Measures: Timely Care Initiation
One OASIS-driven process measure that directly affects TPS is the timely initiation of care. This tracks whether the first skilled visit occurred within two days of the start of care date. Agencies with gaps between referral acceptance and first visit lose points on this measure consistently. For more on how referral speed affects agency performance, see our post on why your referral management process costs you admissions.
How the Scoring and Payment Adjustment Work
CMS calculates your TPS by comparing your performance to all other home health agencies nationally within your size cohort. There are two scoring components: achievement score and improvement score. You receive the higher of the two.
The achievement score measures how well you perform against national benchmarks. The improvement score measures how much you improved from the prior year. Agencies already performing well compete on achievement. Agencies that were previously lower-performing have a path to a positive adjustment through improvement.
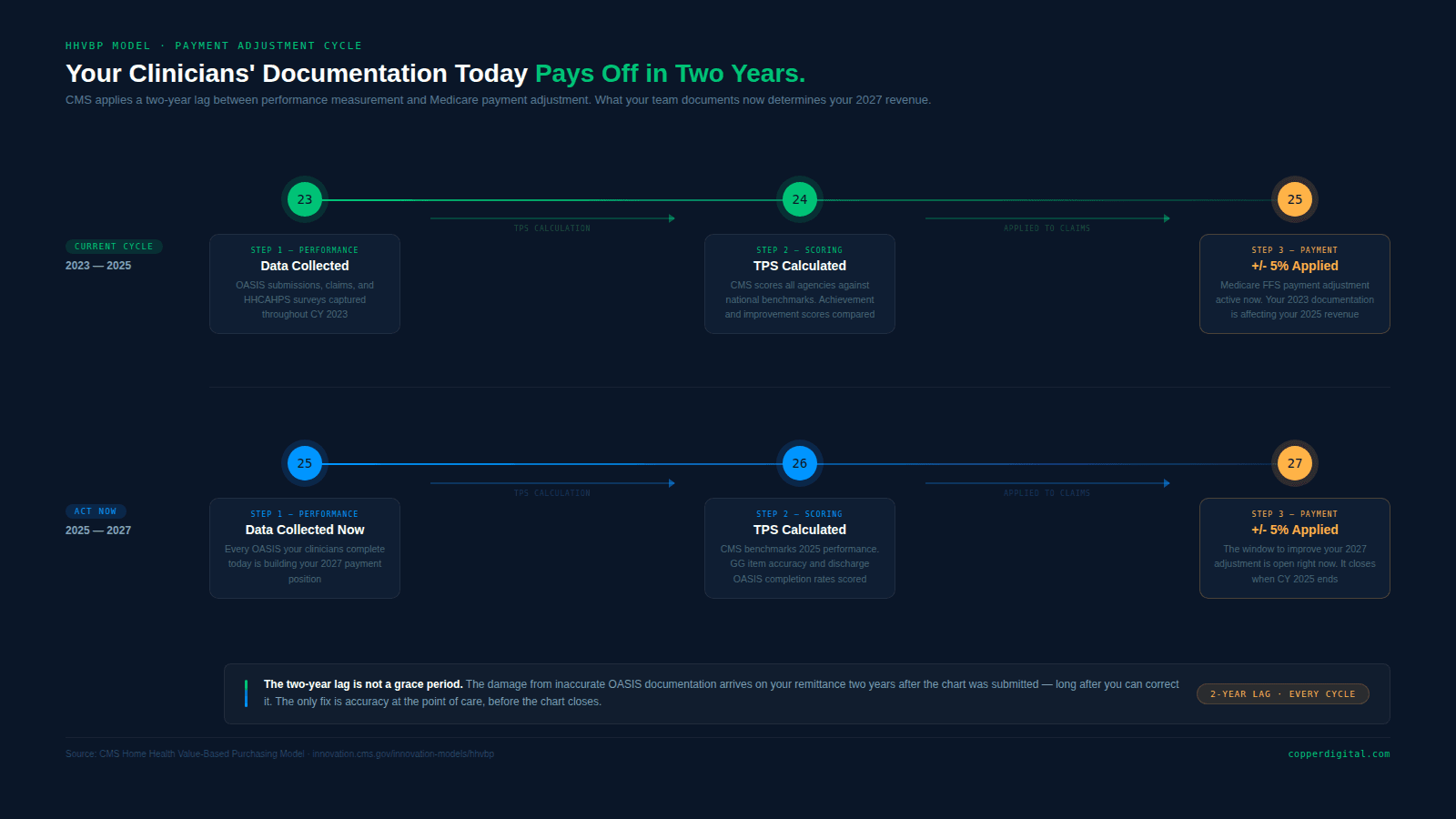
Payment adjustments based on 2023 performance scores are being applied to 2025 Medicare payments. What your clinical team documented two years ago is directly affecting your revenue today. And what they document this year will affect 2027 payments.
The two-year lag between performance and payment means the time to improve OASIS accuracy is always now, not when the adjustment arrives on the remittance.
The Most Common OASIS Accuracy Mistakes That Hurt TPS
Most agencies are not losing TPS points because their clinical care is poor. They are losing points because the documentation does not reflect the care accurately.
Underscoring at Start of Care
Clinicians who err on the side of coding patients as more dependent than they actually are believe they are protecting the agency by creating room to show improvement. The opposite is often true. An underscored SOC sets a lower expected discharge score. When the patient reaches their actual functional level, the improvement looks smaller than it was.
Accuracy at SOC is the foundation of every HHVBP measure. It is not conservative to underscore. It is inaccurate.
Using Activity Not Assessed (ANA) Codes
CMS has flagged overuse of the Activity Not Assessed code on GG items as a significant documentation problem. When ANA is used, CMS imputes a score based on patient characteristics. That imputed score may not reflect the patient's actual status, and it cannot help your Discharge Function Score because there is no observed SOC baseline to compare against.
If a GG item can be assessed, it should be assessed. ANA should be used only when the activity was genuinely not possible to observe or evaluate during the assessment.
Inconsistency Between GG Items and M1800 Items
A patient who scored as requiring maximum assistance for ambulation in the GG mobility items but scored as needing only supervision in the M1800 ambulation item has a documentation inconsistency that will be flagged in any competent QA review. When GG and M1800 items tell different stories about the same patient, the entire assessment loses credibility.
Incomplete Discharge OASIS
The Discharge Function Score requires a discharge OASIS. An agency that discharges patients without a complete OASIS loses the ability to capture the functional improvement that happened during the episode. That improvement existed. It just never made it into the TPS calculation.
Discharge OASIS completion rates are a direct indicator of TPS performance. Agencies with high completion rates capture more of the outcomes they earned.
What Agencies With Strong TPS Scores Do Differently
They train on GG items specifically, not OASIS generally
The shift from M1800-based to GG-based scoring in 2025 required a change in clinician training. Agencies that updated their OASIS education to focus specifically on GG item definitions, the 6-point rating scale, and the distinction between what a patient does versus what they can do are scoring more accurately. Generic OASIS training that does not address GG specifics is insufficient.
They conduct SOC-to-discharge tracking in real time
Rather than waiting for quarterly reports, high-performing agencies track the gap between SOC and discharge GG scores at the patient level throughout the episode. When a patient is not showing expected functional progress, clinicians and care managers are alerted in time to intervene, adjust the plan of care, and document the clinical reasoning.
They use pre-visit automation to reduce cognitive load at SOC
The Start of Care visit is where OASIS accuracy is established and where cognitive load is highest. Clinicians who arrive with a pre-populated chart, referral data already extracted, and prior functional scores already visible are better positioned to assess accurately. Pre-visit automation that prepares the chart before the clinician walks through the door does not replace clinical judgment. It protects it. See our detailed breakdown in how to reduce OASIS documentation time in home health.
They integrate QA into the workflow, not after it
Post-visit QA that catches errors three days after the SOC is less effective than real-time QA that flags inconsistencies before the chart is closed. Agencies using documentation tools with built-in guardrails catch and correct errors before they affect the TPS. This is also why AI-powered agents outperform traditional RPA in home health workflows: rule-based scripts cannot reason about clinical inconsistency the way an AI agent can.
What to Do With This Information
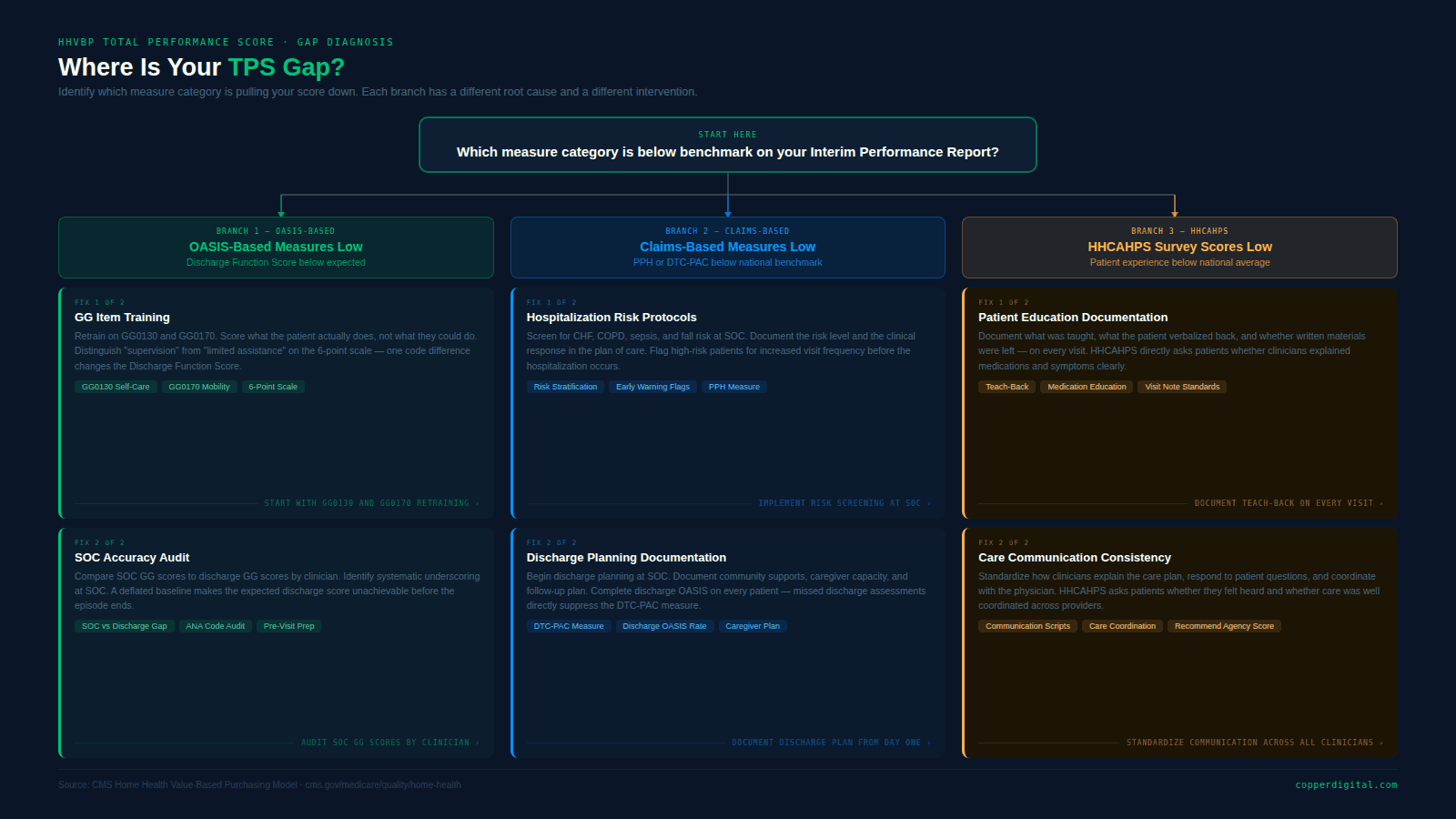
If you are not currently tracking your TPS by measure category, start by pulling your most recent Interim Performance Report from CMS. Identify whether your gaps are in OASIS-based measures, claims-based measures, or HHCAHPS. For a full picture of your 2025 compliance obligations alongside HHVBP, see our 2025 home health compliance and interoperability guide.
If your OASIS-based measure scores are below benchmark, the root cause is almost always one of three things: GG item training gaps, SOC underscoring, or incomplete discharge OASIS. All three are solvable with the right combination of clinical education and documentation workflow.
If your claims-based measures are the gap, the focus shifts to care planning quality, hospitalization risk identification, and discharge planning documentation.
If HHCAHPS is the gap, the focus is on whether specific clinical conversations are happening consistently and being documented in a way that reinforces the practice.
Frequently Asked Questions
What is the HHVBP Total Performance Score?
The Total Performance Score is the composite score CMS uses to calculate your annual HHVBP payment adjustment. It is built from three measure categories: OASIS-based outcomes, Medicare claims-based outcomes, and HHCAHPS patient survey results. Your score determines whether you receive a payment bonus of up to five percent, no adjustment, or a payment reduction of up to five percent on your Medicare fee-for-service revenue.
Which OASIS items have the biggest impact on HHVBP in 2025?
The GG functional items, specifically GG0130A through GG0130C and GG0170A through GG0170R, have the highest direct impact on the Discharge Function Score, which is the primary OASIS-based measure driving the TPS in 2025. These items replaced the M1800 series as the basis for functional outcome scoring. Full instrument specifications are available on the CMS OASIS data sets page.
How does underscoring at Start of Care affect HHVBP?
When clinicians score patients as more functionally impaired than they actually are at Start of Care, the risk-adjusted expected discharge score is set too low. When the patient reaches their actual functional level by discharge, the improvement appears smaller than it was. This reduces the Discharge Function Score and can result in a lower TPS, even when the clinical care was excellent.
Can automation improve HHVBP scores?
Automation improves HHVBP scores indirectly by reducing the cognitive burden on clinicians at Start of Care, which is when the most critical OASIS scoring decisions are made. When pre-visit preparation is handled automatically, clinicians can focus on accurate functional assessment rather than simultaneous data entry. Automation also supports real-time QA that catches scoring inconsistencies before they are submitted. See how this works in practice in our post on reducing OASIS documentation time.
When do 2025 OASIS scores affect Medicare payments?
Under the HHVBP model, there is a two-year lag between performance and payment adjustment. Performance data collected in 2025 will be used to calculate payment adjustments applied in 2027. Improving OASIS accuracy today has a real financial return, but that return will appear on the remittance advice two years from now.
Ready to See How Copper Digital Supports HHVBP Performance?
Copper Digital's pre-visit automation pre-populates OASIS fields from referral documents before the clinician's first visit. Built-in documentation guardrails flag GG item inconsistencies in real time. QA workflows surface incomplete discharge assessments before the episode closes.
If OASIS accuracy is where your TPS gap lives, that is exactly what we are built to address.
Book a Demo →

