Blog
Mar 5, 2026
The Face-to-Face Documentation Problem Is a Workflow Problem

Arvind Sarin

The face-to-face encounter requirement has been part of home health Medicare certification since 2011. It is one of the most frequently audited documentation elements in home health, and it is one of the most consistently incomplete in the agencies that face recoupment. Not because agencies are unaware of the requirement. Because the documentation that gets produced for it almost never says what CMS actually needs it to say.
This post explains what the face-to-face requirement actually requires, what makes a compliant encounter note, the specific failure patterns that generate ADR denials, and what needs to change upstream to get this right before the ADR arrives.
What the Face-to-Face Requirement Actually Is
Under Medicare home health regulations, a physician or allowed non-physician practitioner must conduct a face-to-face encounter with the patient before certifying home health eligibility. The encounter must occur within a defined timeframe, the documentation of that encounter must be part of the medical record, and the documentation must demonstrate that the clinical findings support home health eligibility.
The requirement exists for a specific reason: CMS wants evidence that a clinician actually examined the patient and determined that skilled care and homebound status were warranted. A phone order, a signed certification form without clinical narrative, or a note that simply states the patient needs home health does not satisfy that intent. The encounter documentation must show that an examination happened and that the findings justify home health services.
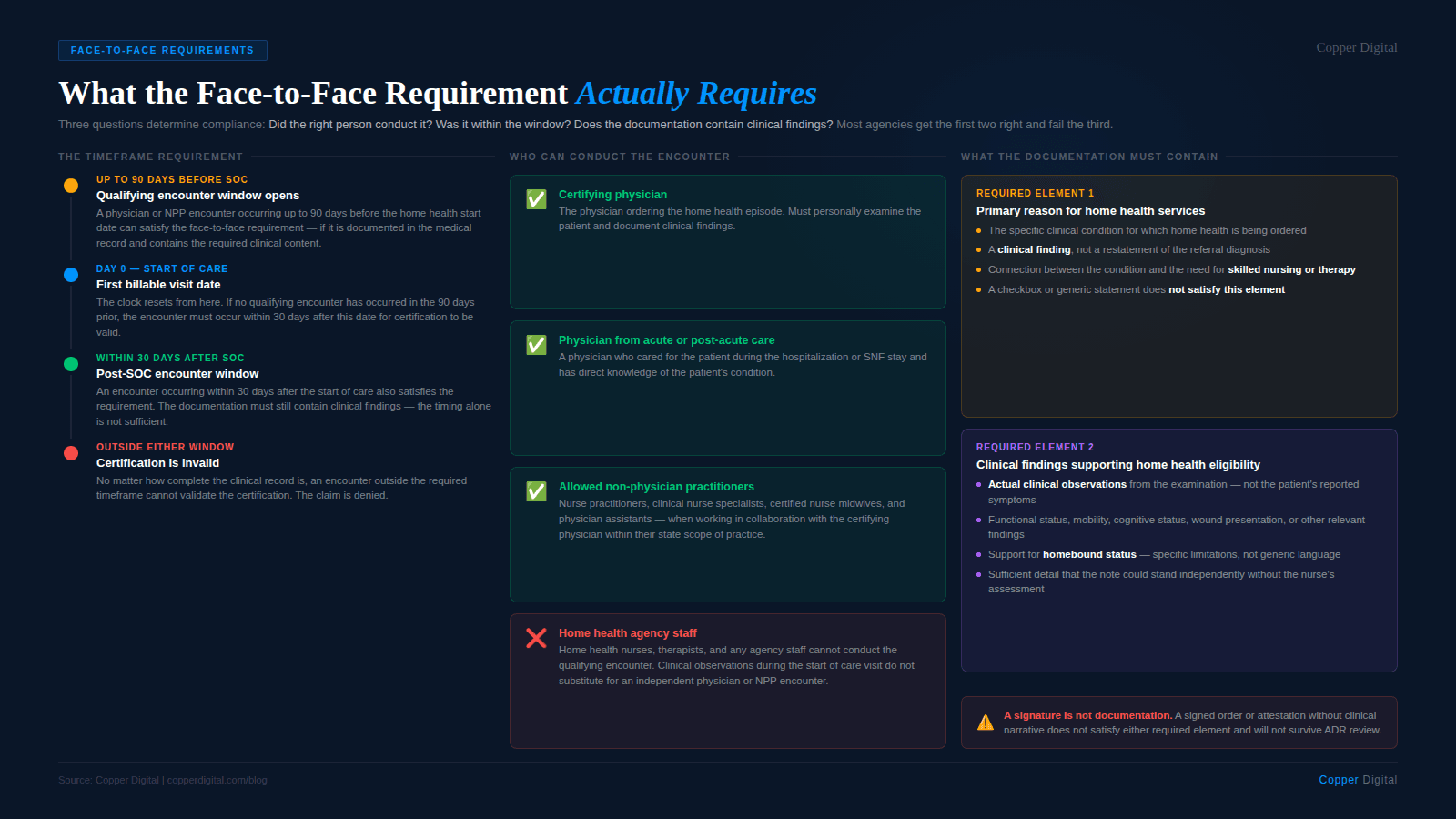
Who can conduct the encounter
The face-to-face encounter can be conducted by the certifying physician, a physician who cared for the patient in an acute or post-acute setting and has knowledge of the patient's clinical condition, or an allowed non-physician practitioner. Allowed NPPs include nurse practitioners, clinical nurse specialists, certified nurse midwives, and physician assistants, but only when working in collaboration with the certifying physician and within the scope of their practice and applicable state law.
The encounter cannot be conducted by a home health nurse, a home health therapist, or any member of the home health agency staff. If the home health clinician documents observations during the start of care that are then used to support certification without an actual physician or NPP encounter having occurred within the required timeframe, that is a compliance failure.
The timeframe requirement
The face-to-face encounter must occur no more than 90 days before the start of the home health episode or within 30 days after the start of the home health episode. The clock starts from the first billable visit date. If the encounter falls outside this window, the certification is not valid regardless of how complete the documentation is.
Telehealth and face-to-face CMS has allowed telehealth encounters to satisfy the face-to-face requirement under certain conditions, a policy that expanded significantly during and after the COVID-19 public health emergency. Agencies should confirm the current CMS guidance on telehealth-based face-to-face encounters, as the applicable rules have changed over time and may continue to evolve. A telehealth encounter that meets the requirements counts as a valid face-to-face — but the documentation requirements for what the encounter must contain are the same regardless of modality. |
What the Face-to-Face Documentation Must Contain
This is where most agencies fail. The timeframe is met. The encounter happened. But the documentation produced by the physician or NPP does not contain the elements that CMS requires for the certification to be valid.
The face-to-face documentation must contain two specific elements:
The primary reason for home health services. The documentation must identify the primary condition for which the patient is receiving home health care. This must be a clinical finding, not a restatement of the referral diagnosis. It should connect the condition to the need for skilled nursing, physical therapy, speech-language pathology, or occupational therapy.
The clinical findings supporting home health eligibility. The documentation must include the clinical findings from the encounter that support both the patient's homebound status and the need for skilled care. This means actual clinical observations — functional status, mobility limitations, cognitive status, wound presentation, medication complexity, or other findings that justify home health services.
Neither of these elements can be satisfied by a checkbox, a signature, or a generic statement. The documentation must contain specific clinical content that could stand independently as evidence that an examination occurred and that the findings support home health eligibility.
A face-to-face note that says 'patient is homebound and requires skilled nursing' tells an auditor nothing. A face-to-face note that describes what the physician observed in the examination and connects those observations to specific functional limitations and skilled care needs — that is documentation that holds. |
The Five Face-to-Face Documentation Failures
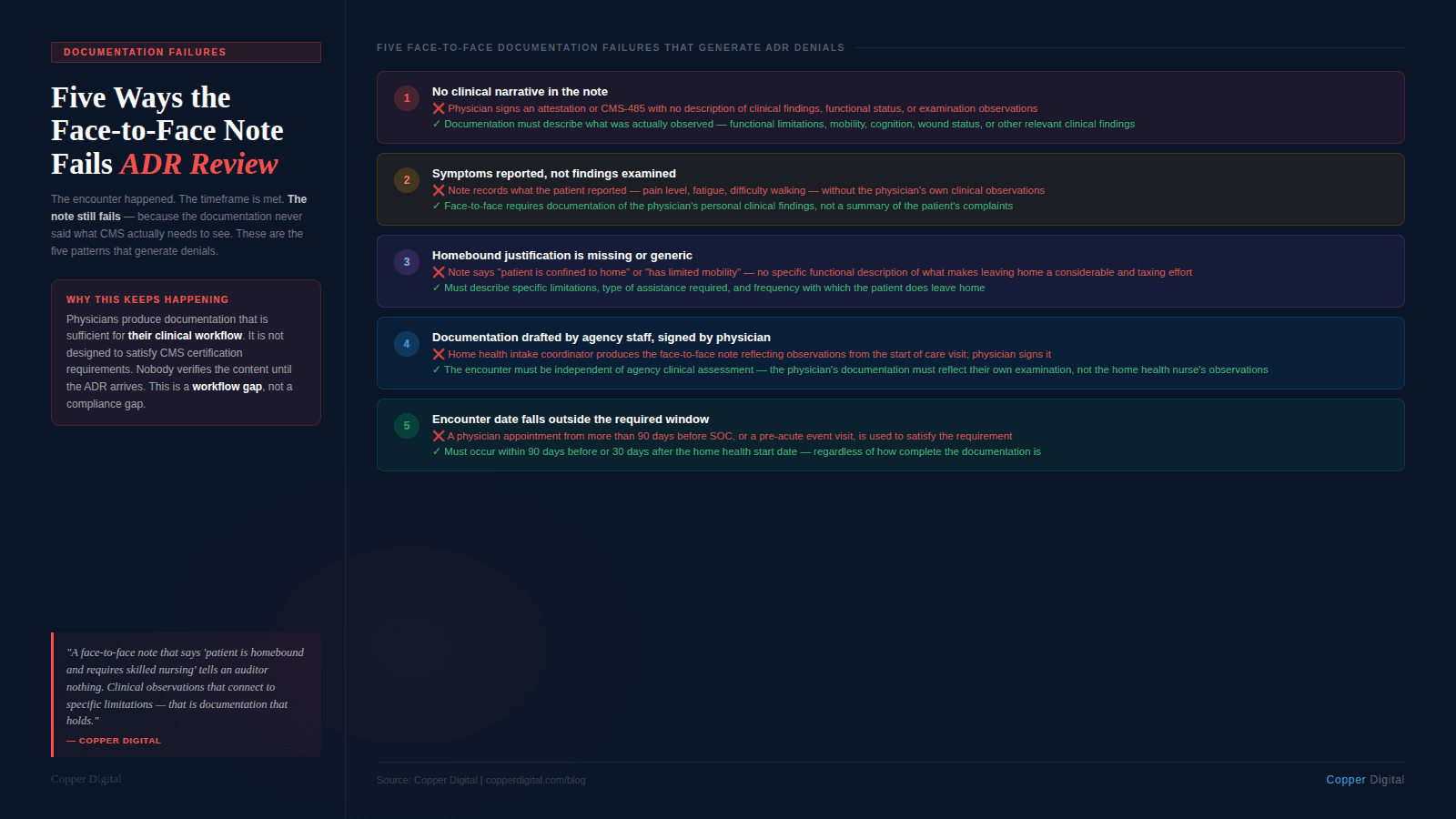
Based on CMS audit findings and MAC guidance, these are the specific documentation patterns that result in face-to-face related denials:
1. The encounter note has no clinical narrative
The most common failure. The physician signs a CMS-485 or a brief attestation stating that the patient was seen and home health is recommended. There is no description of what was observed during the examination, no functional status information, and no connection between clinical findings and the home health need. This does not satisfy the requirement. A signature is not documentation.
2. The documentation describes what the patient reports, not what was examined
A face-to-face note that records the patient's reported symptoms — pain level, fatigue, difficulty walking — without describing the physician's own clinical observations is insufficient. The requirement is for documentation of clinical findings from an examination, not a summary of the patient's complaints. The physician or NPP must document what they personally observed and assessed.
3. The homebound justification is missing or generic
The face-to-face documentation must support homebound status. A note that says the patient is confined to the home or has limited mobility does not meet this standard. The documentation must describe the specific functional limitations that make leaving home a considerable and taxing effort. This connects directly to the homebound documentation requirements that govern the overall home health certification.
4. The encounter is documented by home health agency staff
Some agencies — particularly when coordinating with physician practices that have limited administrative capacity — produce face-to-face documentation that was drafted by the home health intake coordinator or clinical supervisor and then signed by the physician. If the documentation reflects observations made during the home health start of care visit rather than a separate physician or NPP encounter, it is not a valid face-to-face. The encounter must be independent of the home health agency's own clinical assessment.
5. The encounter date falls outside the required window
A physician appointment documented in the hospital discharge record that occurred more than 90 days before the home health start date does not satisfy the requirement. A primary care visit that occurred before the acute event that precipitated the home health referral does not satisfy the requirement. The encounter must occur within the defined timeframe relative to the home health start date, and agencies must verify this before submitting the certification.
The Upstream Problem: Why This Keeps Happening
Face-to-face documentation failures are almost never intentional. They reflect a structural gap between what the home health agency needs from the physician and what the physician's documentation workflow actually produces.
Most physicians certifying home health services are not home health specialists. They are primary care physicians, hospitalists, or specialists managing a broad patient population. The specific documentation requirements for home health face-to-face certification are not part of standard clinical documentation training. When a physician dictates a brief note confirming that the patient was seen and agrees with the home health plan, that is a reasonable clinical workflow for their purposes. It is not sufficient for home health certification purposes.
The gap is that the home health agency receives a referral and a signed physician order, assumes the face-to-face documentation requirement is being handled by the physician's office, and proceeds to intake. The physician's office assumes the home health agency will manage any additional documentation requirements. The face-to-face note that ends up in the record is whatever was in the physician's standard dictation workflow, which was never designed to satisfy CMS certification requirements.
By the time the ADR arrives, the physician may no longer remember the encounter clearly, the clinical record from the encounter may be at a different practice or health system, and supplementing the face-to-face documentation after the fact is both procedurally complicated and clinically risky.
The physician does not know what CMS needs from the face-to-face note. The agency assumes the physician is handling it. Nobody checks until the ADR arrives. This is a workflow gap, not a compliance gap — and it has a workflow solution. |
What Compliant Face-to-Face Documentation Looks Like
A compliant face-to-face note does not need to be long. It needs to be specific. Here is what the documentation should contain:
Clinical findings from the examination
Functional status observed during the encounter — can the patient ambulate, transfer, dress, manage medications independently?
Cognitive status assessment — is the patient oriented, able to follow instructions, capable of self-managing care?
Relevant clinical findings — wound presentation if wound care is the primary reason, cardiopulmonary status if cardiac or pulmonary management is the focus, neurological status if neuro conditions are relevant
Any safety concerns observed — fall risk, medication management risk, environmental concerns
Homebound status support
Description of the specific limitations that make leaving home a considerable and taxing effort
Type and level of assistance required to leave home — person assistance, mobility equipment, transportation arrangement
Frequency with which the patient does leave home and the nature of those absences
Primary reason for home health services
The specific clinical condition that is the primary reason for the home health episode
Connection between that condition and the need for skilled nursing, therapy, or both
Why the skilled service cannot be safely and effectively provided in a non-home setting given the patient's functional status
Providing a face-to-face documentation template to referring physicians Many agencies have success providing referring physicians with a structured template or checklist that captures the required elements while fitting within a standard documentation workflow. The template prompts the physician to document functional status, homebound justification, and the primary reason for home health in enough clinical detail to satisfy CMS requirements. This is not ghost-writing — the physician must complete and sign it based on their own clinical findings. It is giving the physician a structure that produces compliant documentation rather than assuming their standard workflow will. |
How AI-Assisted Workflows Address the Face-to-Face Gap
The face-to-face problem is a coordination and tracking problem. The agency needs documentation from a physician or NPP that meets specific content requirements, within a specific timeframe, and the agency typically has limited control over when or how that documentation is produced. AI-assisted intake workflows address this in two ways.
Proactive gap detection at intake
At the time of referral, an AI-assisted intake workflow can identify whether the face-to-face documentation requirement has been satisfied. It can check the referral documentation for a qualifying encounter within the required timeframe, flag cases where the encounter date or documentation is missing, and trigger an outreach to the referring physician's office before the episode begins. This is the same logic that makes PDGM diagnosis extraction at intake valuable — getting the right information before the episode starts rather than discovering the gap at ADR response time.
Content validation before certification submission
Before the certification is submitted, an AI validation check can review the face-to-face documentation against the required content elements — is there clinical narrative, is there homebound justification, is there a primary reason statement, is the encounter date within the required window. Cases where the documentation is insufficient flag for human review before submission. This is a pre-submission audit that catches the failure before the MAC does.
The same logic applies to the internal consistency check described in our ADR defense post: face-to-face documentation should be consistent with the OASIS functional assessment and the primary diagnosis coding. A face-to-face note that describes a patient as fully functional while the OASIS records significant limitations creates the kind of contradiction that triggers automated review flags.
Face-to-Face Documentation Checklist
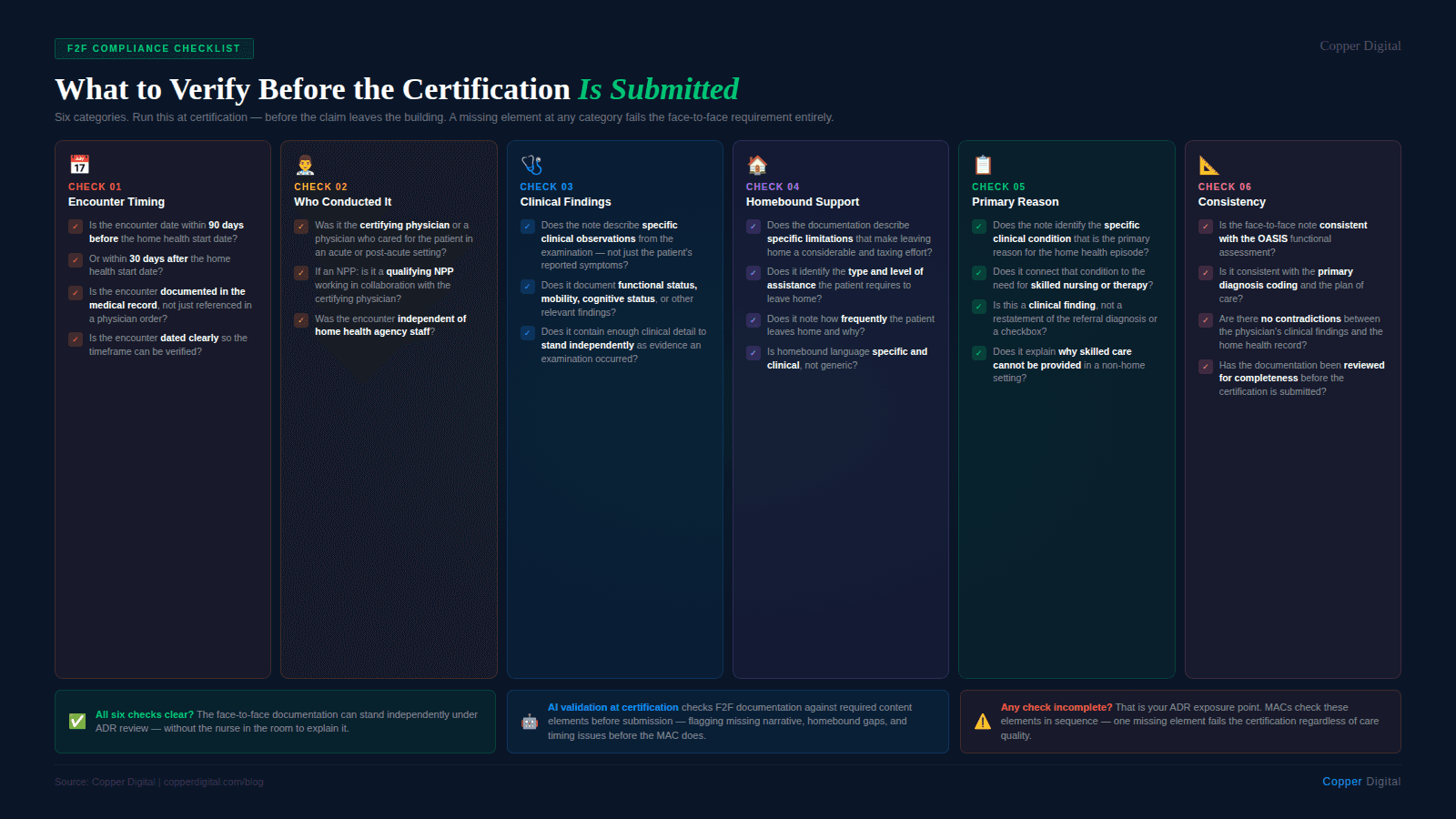
Use this checklist at certification to verify the face-to-face requirement is met before submitting the claim.
Timing
Is the encounter date within 90 days before or 30 days after the home health start date?
Is the encounter documented in the medical record, not just referenced in a physician order?
Who conducted the encounter
Was the encounter conducted by the certifying physician, a physician with knowledge of the patient's condition from an acute or post-acute setting, or an allowed NPP?
Was the encounter independent of the home health agency's own clinical assessment?
Content: clinical findings
Does the documentation describe specific clinical observations from the examination — functional status, mobility, cognitive status, wound presentation, or other relevant findings?
Does it contain the physician's or NPP's own clinical observations, not just the patient's reported symptoms?
Content: homebound justification
Does the documentation describe specific limitations that make leaving home a considerable and taxing effort?
Does it identify the type and level of assistance the patient requires to leave home?
Content: primary reason for home health
Does the documentation identify the primary clinical condition for which home health is being ordered?
Does it connect that condition to the need for skilled nursing or therapy services?
Consistency
Is the face-to-face documentation consistent with the OASIS functional assessment and the primary diagnosis coding?
Are there any contradictions between the face-to-face clinical findings and the home health record that would raise questions about the validity of either document?
Copper Digital's AI-assisted intake workflow checks face-to-face documentation against required content elements before certification is submitted — flagging missing clinical narrative, homebound justification gaps, and timing issues before they become ADR denials. Request a demo to see how this works in your agency's intake process. |
Related Reading
Why Home Health Agencies Fail ADR and TPE Audits: It Is Not the Care. It Is the Documentation.
Homebound Status Documentation: What It Must Say and What It Must Not Leave Out
How Medicare Bots Find the Errors Humans Miss in OASIS Documents
An Autopsy of a Start of Care: The 2-Hour Visit That Takes 6 Hours

