Blog
Jan 20, 2026
Your Intake Process is Poisoning Your Clinical Data

Arvind Sarin
We often blame the field nurse for documentation errors.
When a chart comes back with conflicting data, we assume the clinician made a mistake in the home. We assume they didn't look at the wound closely enough, or they forgot to ask about the fall history.
But what if the error didn't happen in the home?
What if the error had occurred three days earlier, when a PDF arrived in your inbox?
The most dangerous moment in a patient's lifecycle is not the Start of Care visit. It is the moment a human intake coordinator opens a 50-page hospital referral and starts typing it manually into your EMR.
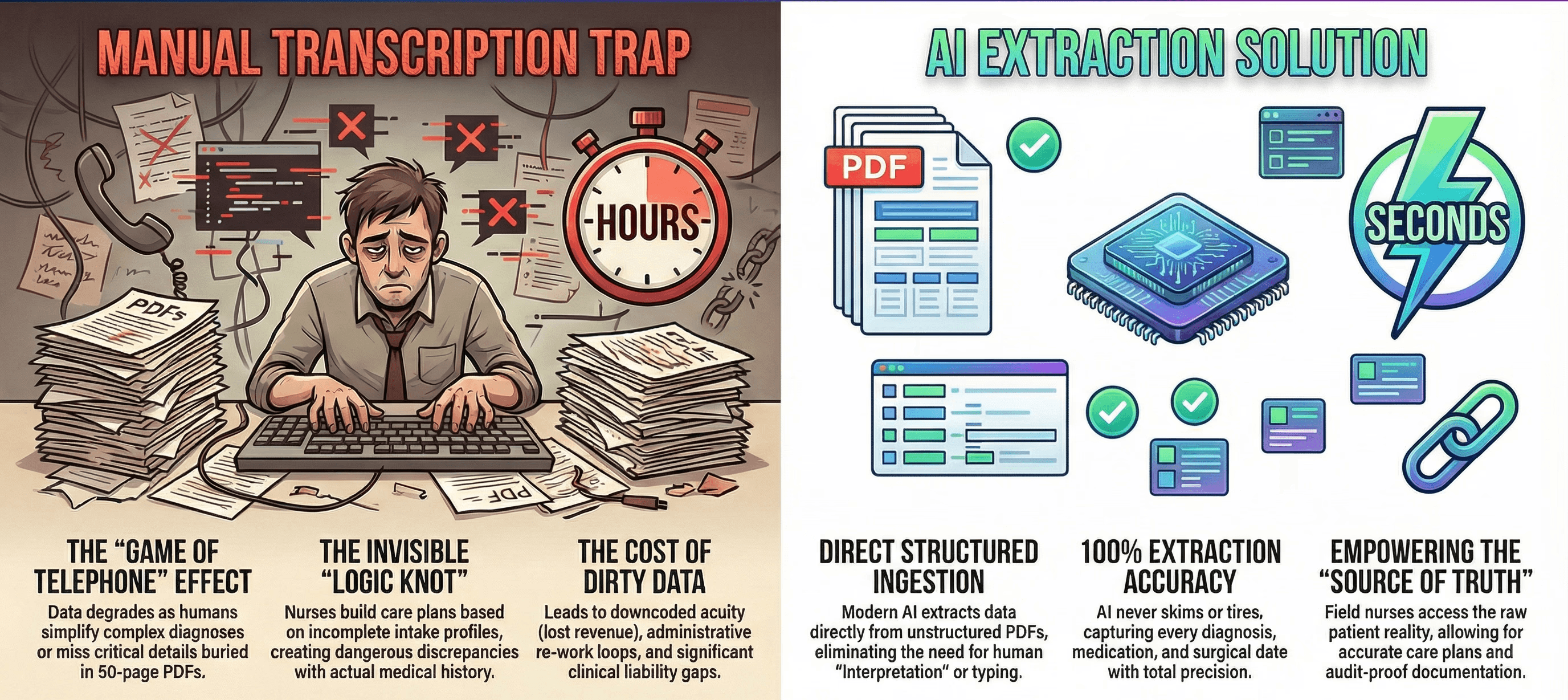
We call this the Transcription Trap. It is an invisible filter that distorts clinical reality before your nurse ever starts their car.
The Game of Telephone
Think about how a patient reaches your agency.
They are discharged from a hospital with a complex digital record. That record is printed to a PDF and faxed to your office. A human being then reads that PDF and manually re-enters the data into your software.
This is a high-stakes game of Telephone.
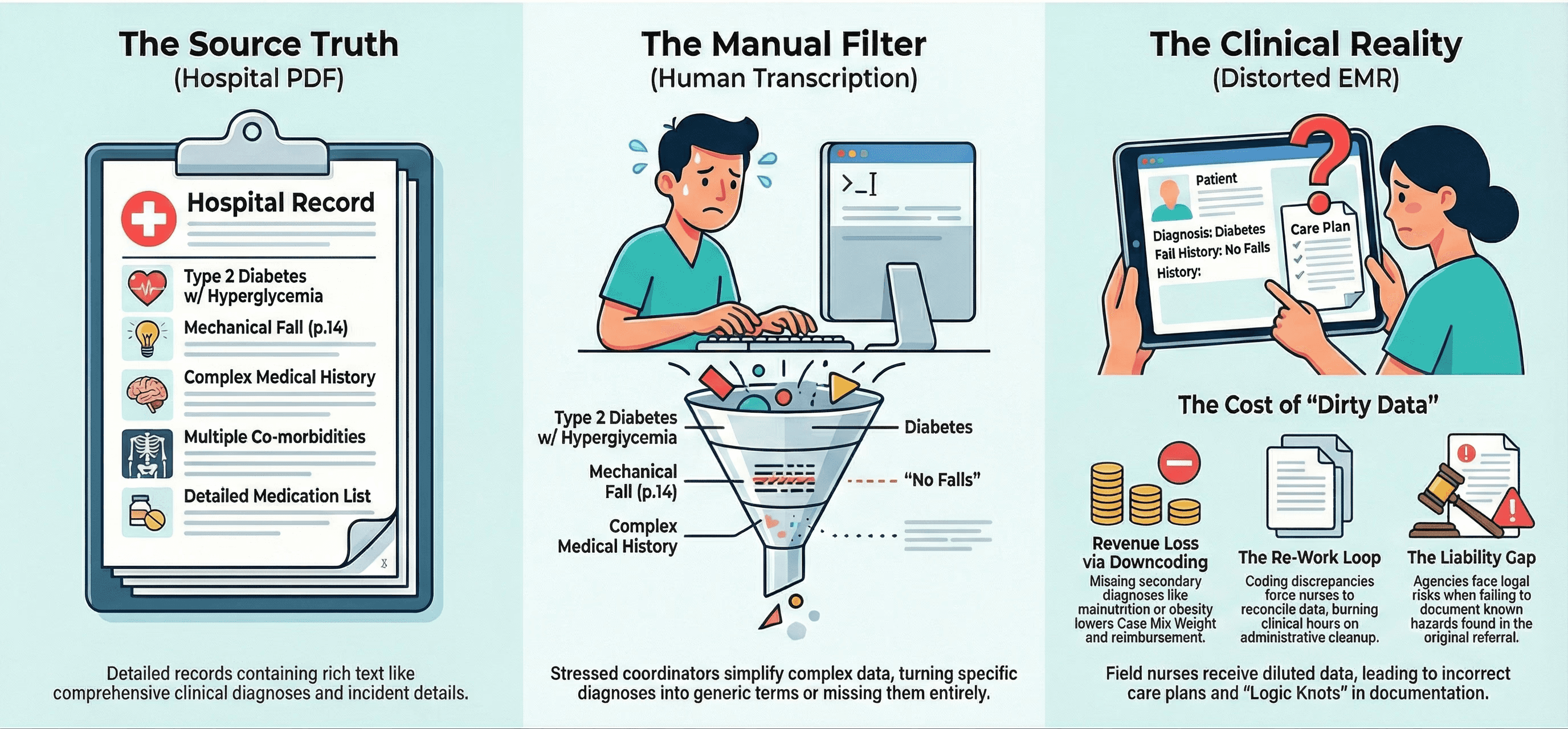
Every time data moves from one format to another, it degrades. A specific diagnosis code like "Type 2 Diabetes with Hyperglycemia" gets simplified to just "Diabetes" by a rushed intake coordinator. A complex surgical history gets shortened to fit a text box.
By the time the data reaches the field nurse, it has been diluted.
The nurse trusts this data. She sees "No History of Falls" in the intake profile and assumes it is true. She builds her care plan based on that fact.
But the original hospital discharge summary actually noted a "mechanical fall" on page 14. The intake coordinator simply missed it.
Now you have a Logic Knot in your chart. The nurse documents "Safe Ambulation" because she trusts the intake data. But the hard evidence says the patient is a fall risk.
The Illusion of Continuity
We like to believe we have "Continuity of Care." In reality, we have "Continuity of Data Entry."
A study by the American Health Information Management Association (AHIMA) found that manual data entry is a primary source of patient matching errors and clinical discrepancies.
When your intake team manually enters a medication list, they are not just typing. They are interpreting.
They see "Lasix 40mg" on the discharge list. But they don't see the renal failure diagnosis buried in the lab results. They enter the drug but miss the context.
Your nurse walks in blind. She sees the medication but not the risk factor. She might grade the patient's management ability as "Independent" because she doesn't know the complexity of the regimen.
This is how you fail a Start of Care audit before the visit even begins.
The Cost of Dirty Data
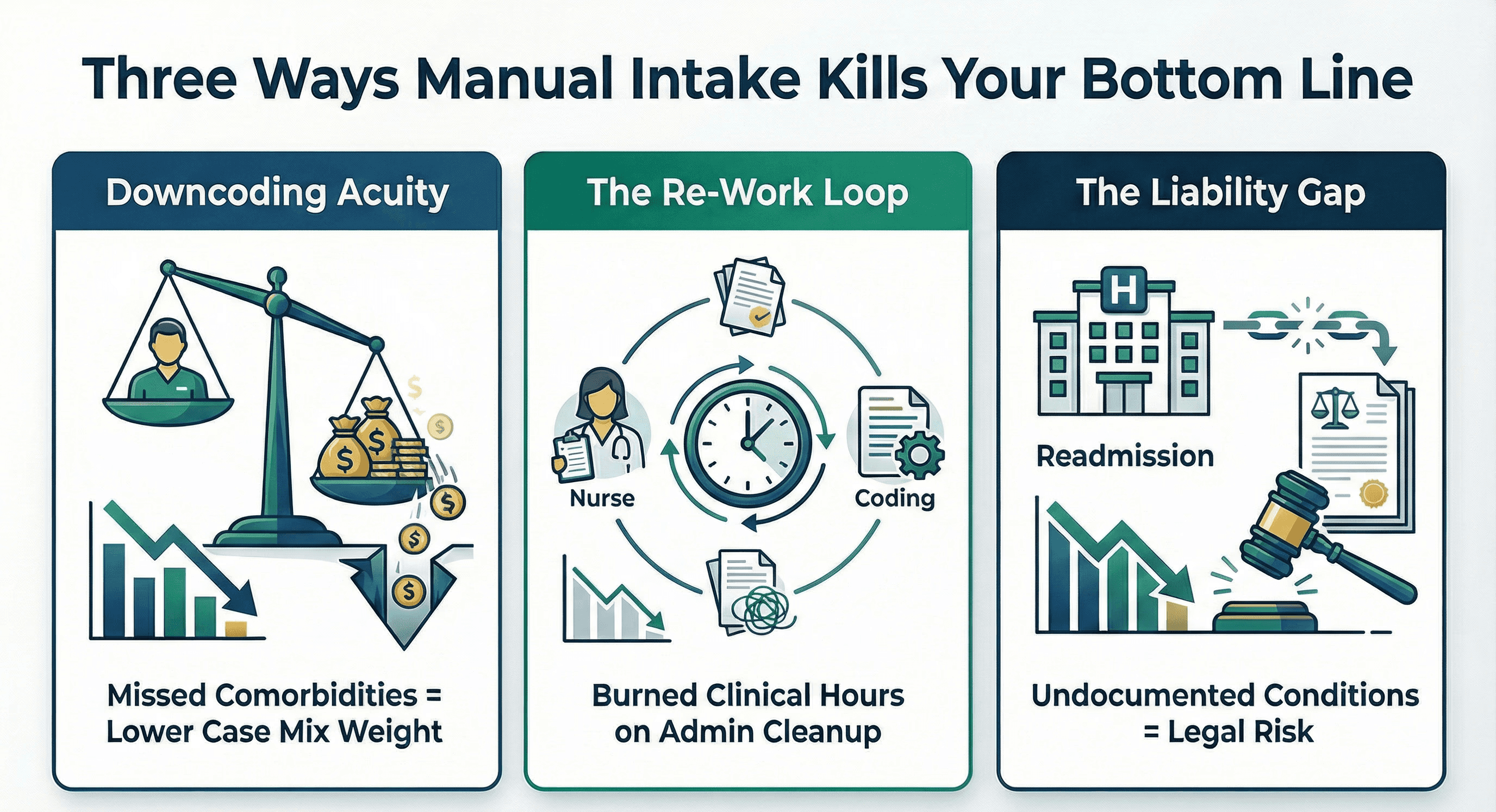
This poisoned data stream destroys your revenue cycle in three specific ways.
1. Downcoding Acuity
If the intake coordinator misses a secondary diagnosis like "Malnutrition" or "Morbid Obesity," your nurse likely will too. These comorbidities drive your Case Mix Weight. If they don't make it from the PDF to the EMR, you are doing the work for free.
2. The Re-Work Loop
Your coding team eventually catches these mismatches. They see the discrepancy between the hospital referral and the OASIS. They kick the chart back to the nurse. Now the nurse has to reconcile data she didn't even enter. This burns valuable clinical hours on administrative cleanup.
3. The Liability Gap
If a patient is readmitted to the hospital for a condition you failed to document, you have a liability problem. You cannot claim you didn't know. The information was right there in the referral. Your process just failed to extract it.
Stop Typing and Start Extracting
The solution is not to hire more intake coordinators. Adding more humans to a manual process just adds more potential for error.
The solution is to remove the manual transcription step entirely.
Modern AI does not "read" a referral like a human does. It ingests it. It extracts structured data directly from the unstructured PDF.
It doesn't get tired. It doesn't skim past page 40. It finds every diagnosis and every medication, and every surgical date with 100 percent accuracy.
It populates your Start of Care assessment with the raw truth from the hospital.
When your nurse opens the chart, she isn't looking at a summary typed by a rushed coordinator. She is looking at the source of truth.
She sees the fall history. She sees the renal failure. She sees the complexity.
This allows her to grade Performance rather than Capacity. She can build a care plan that reflects the actual patient reality.
Your clinical data is the lifeblood of your agency. Stop letting a manual intake process poison the well.
Clean your data at the source.

