Blog
Apr 13, 2026
The Family Caregiving Crisis in the USA: Why the System Is Failing Them

Dr. Pooja Patel | Founder, Aging Together
When I was working in the hospital, I spent a lot of time watching the same scene play out. Someone comes in, usually older, usually after a fall or an infection or a cardiac event. We stabilize them. And then, within 24 to 48 hours, a family member walks in, overwhelmed and sleep-deprived, and we offload an enormous amount of information onto them. Medication changes. Discharge recommendations. Equipment needs. A decision about whether to go to inpatient rehab, a skilled nursing facility, or home with home health. Sometimes we hand them paperwork. Sometimes we connect them with a social worker. Rarely do we have the time to make sure they actually understood any of it.
And here is the part I kept getting stuck on: most of these families had no idea any of this was coming. They had never thought about what happens when a parent can no longer manage on their own. They did not know what home health covers and what it does not. They did not know the difference between an assisted living facility and a skilled nursing facility. They did not know what questions to ask, what to look for, or what to avoid. And they had 24 hours to make decisions that would significantly affect their family member's quality of life.
That is why I started Aging Together. Not because the health system is broken, though parts of it are, but because the gap in literacy about how this system works is enormous, and most families do not encounter it until they are already in crisis.
The 53 Million People Nobody Talks About
There are currently at least 53 million unpaid family caregivers in the United States. That number is a few years old, so it has likely grown. These are adult children, spouses, siblings, friends, and neighbors who are managing medications, driving to appointments, handling finances, preparing meals, assisting with bathing and dressing, and often doing all of this while also working full-time jobs, raising their own children, and managing their own health.
They are not counted in the healthcare workforce. They are not reimbursed. They are not trained. And they are routinely handed responsibilities that clinical professionals spend years learning to manage.
In the field, we say family caregivers are the backbone of care in America. It is not a metaphor. If every family caregiver in the United States stopped tomorrow, the hospital system, the nursing home system, and the home health system would be able to absorb the demand. The infrastructure would collapse. We are, as a country, completely dependent on unpaid family labor to hold our care systems together, and we invest almost nothing in supporting the people doing that work.
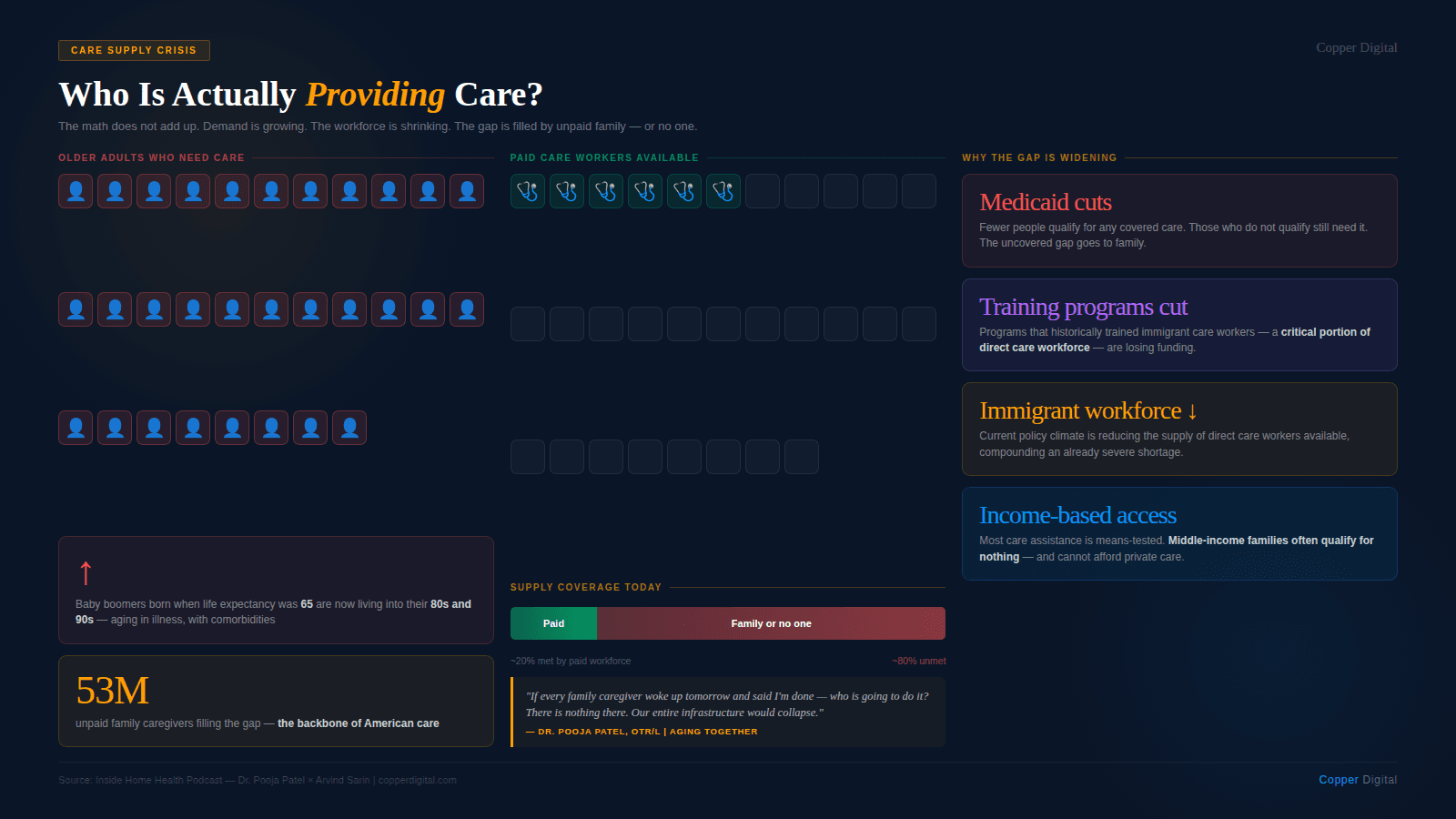
If every family caregiver in the United States stopped tomorrow, our entire care infrastructure would collapse. We know this. And yet we invest almost nothing in preparing or supporting the people doing that work. |
We Are Living Longer but Not Better Prepared
When the first baby boomers were born, the life expectancy in the United States was 65. Baby boomers are now living well into their 80s and 90s. That is a remarkable achievement. But no one prepared them, or their families, for what those extra decades would actually look like.
This current generation of older adults is aging in illness. They have comorbidities, chronic diseases, and cognitive decline. They need support. And the supply of trained, paid care workers to provide that support is nowhere near adequate to meet the demand. What we have instead is a patchwork system: some coverage through Medicare and Medicaid for those who qualify, some paid care for families who can afford it, and everything else falls to whoever happens to be available in the family.
The families who end up doing this work are often not the ones who volunteered for it. They are the ones who were closest, or the ones who felt the most obligated, or the ones who simply did not have the resources to pay for professional care. And they are doing an extraordinarily demanding job with almost no preparation and no ongoing support.
The information problem
Part of what makes caregiving so difficult is the sheer volume of information you are expected to absorb, retain, and act on, often during the worst moments of your life. When a parent is hospitalized, the family is hearing for the first time about discharge planning, insurance coverage, therapy recommendations, equipment needs, and long-term care options. They are hearing terms they have never encountered. They are expected to make decisions quickly. And they are doing all of this while also being emotionally devastated.
What I see consistently in my work is that the gap is not one of intelligence or caring. The families I work with love their family members deeply and are trying their best. The gap is one of preparation. They simply did not know this was coming, and they had no framework for navigating it when it arrived.
What Proactive Care Planning Actually Looks Like
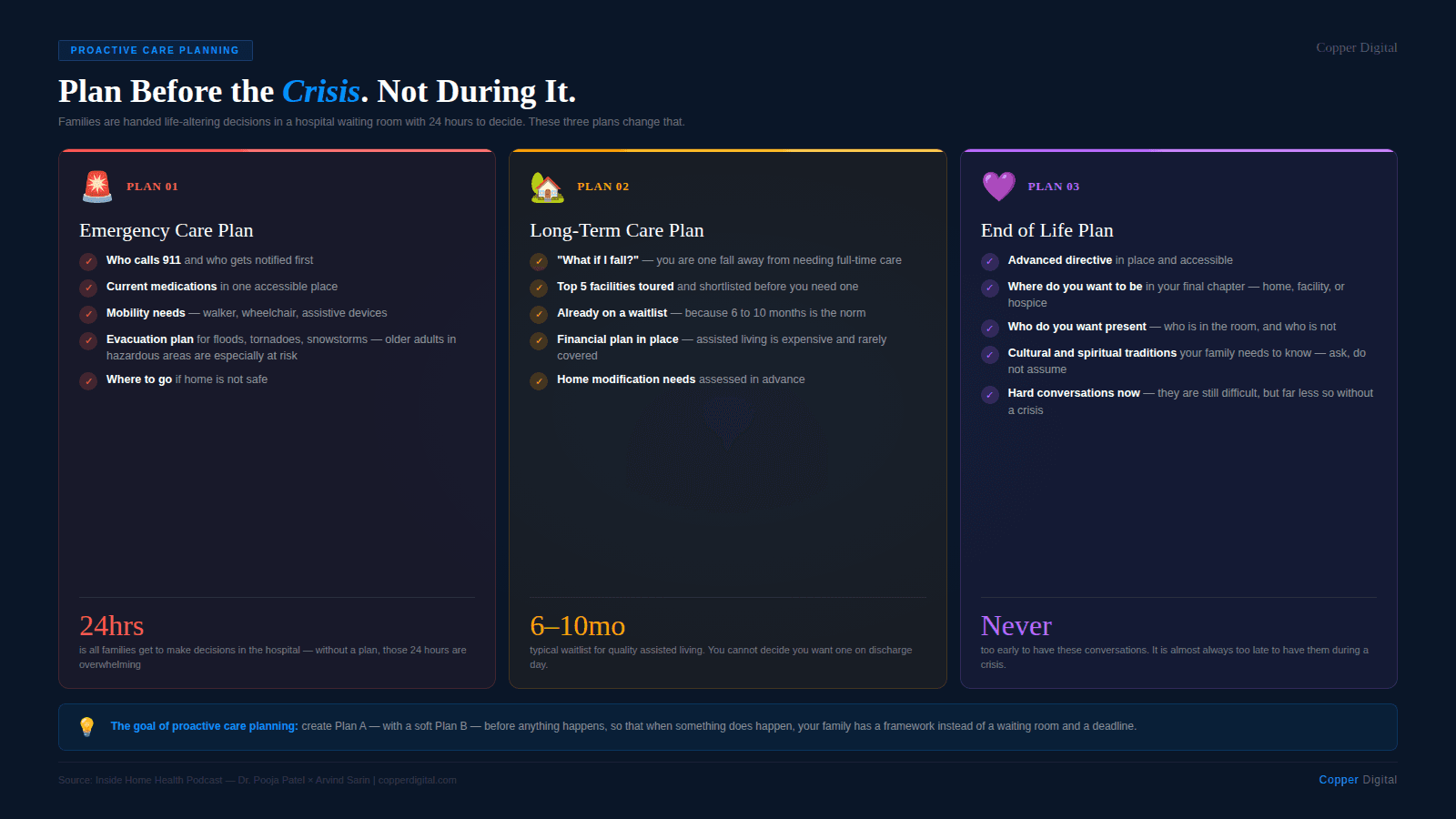
My practice at Aging Together focuses on what I call proactive care planning, or pre-caregiving. The premise is straightforward: you should not be learning how the American care system works while you are in the middle of a crisis. You should be learning it before anything happens, so that when something does happen, you have a plan.
I work with families on three areas of proactive planning.
Emergency care planning
This covers both personal emergencies, such as a fall or a sudden health event, and environmental ones. Older adults who live in areas prone to flooding, wildfires, tornadoes, or snowstorms face a specific and often overlooked risk: if they need to evacuate, do they have a plan? Do they have the mobility equipment they need? Do they know where they are going? Who is responsible for getting them there? These conversations need to happen before the emergency, not during it.
Long-term care planning
A lot of families do not realize how long the waitlists for assisted living facilities can be, or how expensive those facilities are. In the Chicago area where I practice, waitlists run six to ten months at desirable facilities. You cannot be discharged from a hospital and simply decide you want to go to assisted living. That is not how it works. Families who have toured facilities, gotten on waitlists, and made financial plans for this possibility are in an entirely different position than families who have not.
The question I encourage families to think through is: if your parent broke a hip tomorrow and could not return home, what would happen? Do you have a plan? If not, now is the time to make one, not when you are in the emergency department waiting for discharge paperwork.
End-of-life planning
This is the conversation families avoid the most and regret avoiding the most. Beyond the legal documents, the advance directives and powers of attorney, there are practical and deeply personal questions that families need to discuss: How does your parent want to live out their final chapter? Where do they want to be? Who do they want around them? What traditions and rituals matter to them?
I tell families directly: I do not know all the cultural traditions that matter in your family. You might not either. But if your parent has expectations about what those final weeks or months should look like and you have never talked about it, you are both going to be in a very difficult situation. Have the hard conversation now. It will still be difficult. But it will be far less difficult than having it in the middle of a crisis.
You'd rather have those difficult conversations now versus during a time of crisis, because they're still going to be difficult either way. They will be a lot more difficult if there's an active crisis going on. |
The Care Literacy Gap Is Also a Systemic Failure
I want to be clear about something. The families who struggle to navigate this system are not failing. The system is failing them. The American care system is extraordinarily complicated, fragmented, and siloed. The resources that exist, and there are more of them than most families realize, are so poorly connected and communicated that families often cannot find them even when they desperately need them.
I hear people say, just Google it. I want you to try Googling help for aging parents and see what you get. For someone who does not know the difference between home health and home care, who does not know what a certified nursing assistant does versus a home health aide versus a licensed practical nurse, who does not know whether their parent qualifies for Medicaid or what their Medicare plan covers, the results of that search are not going to be helpful. They are going to be overwhelming. Or they are going to lead to a predatory company that is happy to take money from a desperate family.
The resources exist. The collaboration between the professionals who work in this system does not exist at nearly the level it needs to. Care managers, financial advisors, elder law attorneys, occupational therapists, home health agencies, social workers: we are all working with pieces of the same puzzle, and we are not routinely sharing those pieces with each other or with the families who need all of them.
Technology Is Building the Wrong Thing
There has been a significant amount of investment and innovation in healthcare technology over the last decade. Electronic health records, telehealth platforms, remote patient monitoring, and AI-assisted documentation tools. Most of it is built for providers. And I understand why. That is where the reimbursement is. That is where the institutional relationships are.
But the people who actually need help managing the daily complexity of care are not the providers. They are the family caregivers. And right now, most of them are using the notes app on their phone, a paper calendar, and whatever they can remember. They are trying to track medications and medication changes and side effects and appointment schedules and therapy recommendations and insurance authorizations across multiple providers who do not talk to each other and whose systems certainly do not talk to each other. It is an enormous cognitive burden, and it falls almost entirely on people who are also trying to manage their own lives and their own health while doing it. I discussed this directly with Arvind in our conversation, which was recorded for the Inside Home Health podcast series.
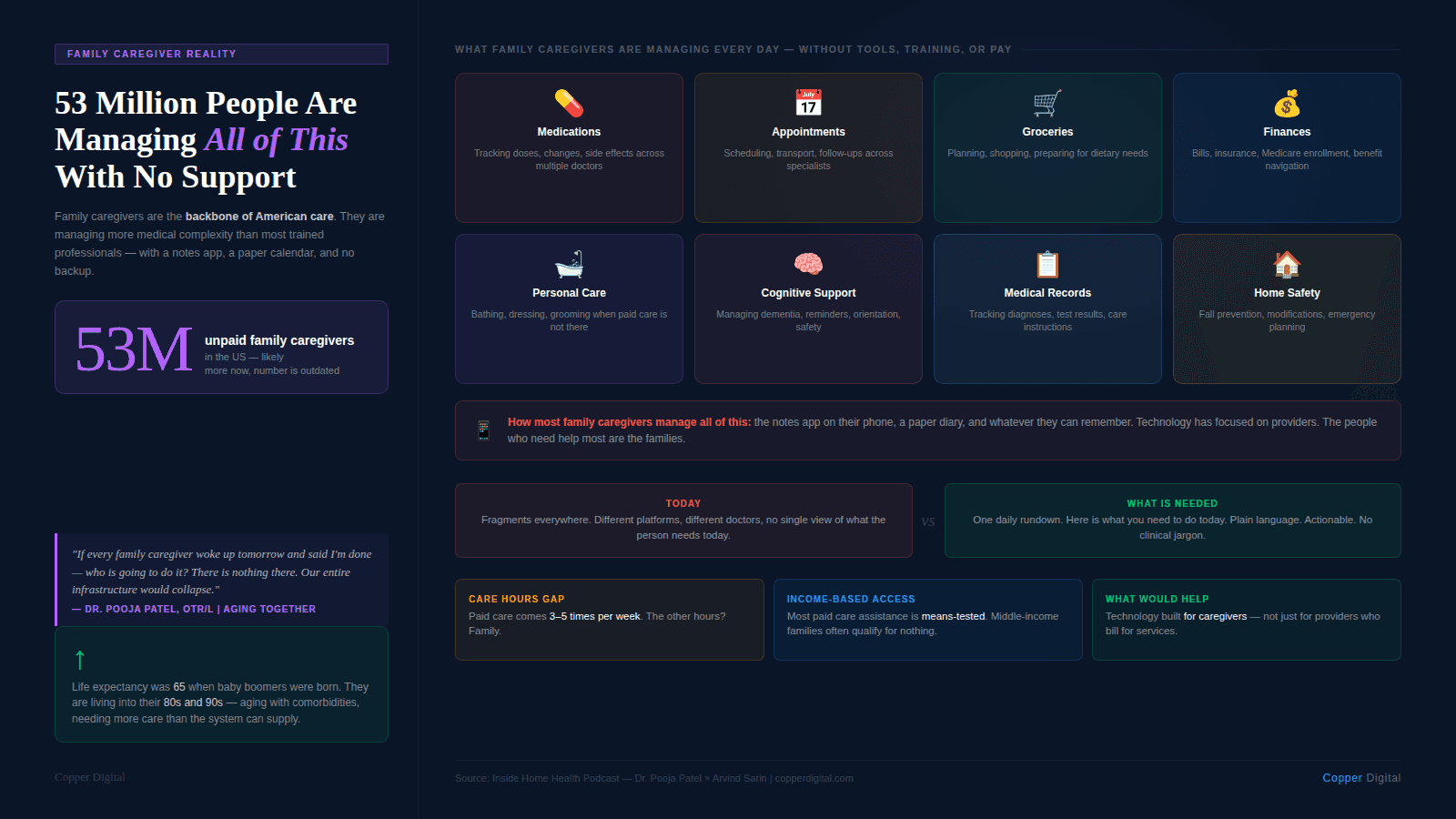
What I would love to see is technology that helps family caregivers the way provider tools are helping providers: streamlining information, surfacing what matters, reducing the cognitive load of managing care day to day. Something that could give a family caregiver a clear daily summary: here is what your parent's care team has said, here is what changed this week, here is what you need to do today. That product does not yet exist in a form that is accessible, affordable, and designed for people who are not themselves clinicians.
Where AI has real potential for caregivers
I am not dismissive of what AI can do in this space. I think there is genuine potential. But it has to be designed for the actual user, which in many cases is an overwhelmed adult child who does not know the medical terminology and does not have time to learn it. The value would be in translation: taking what clinicians know and communicate in clinical language and making it understandable and actionable for the family members who are responsible for carrying out the care between skilled visits.
What Actually Needs to Change
I get asked this question a lot: What do we do? And my honest answer is that there is no single intervention that fixes a system this complex. But there are things that would make a meaningful difference.
Earlier education. Families should not be learning how home health works, how Medicare enrollment works, and what an assisted living facility actually is, for the first time in an emergency room. Healthcare education needs to reach people before a crisis, and it needs to be in a language that people without clinical training can understand.
Better investment in direct care workers. We are losing the workforce that makes home-based care possible. Funding cuts to Medicaid and training programs, combined with the current decline in immigrant care workers who have historically made up a significant portion of this workforce, are creating a supply problem that technology cannot solve by itself.
Cross-sector collaboration. The care professionals who work with families, care managers, elder law attorneys, financial advisors, occupational therapists, and home health agencies need to work together more systematically. Families should not have to piece together the puzzle on their own.
Technology built for caregivers, not just for providers. The people managing the most information with the least support are family caregivers. Investment in tools that actually help them, not just tools that help the professionals who bill for services, would make a real difference.
Honest conversations earlier. In every family. About what aging actually looks like, what care costs, what is covered, what is not, and what each person wants for their own end of life. These are not comfortable conversations. They are necessary ones.
Where to Start If This Is Your Family Right Now
If you are reading this and already in the middle of caregiving without a plan, you are in the majority. Most families arrive at this without preparation, and that is not a personal failure. It is the predictable result of a system that does not prepare people for it.
Start with what you can do this week. Have one conversation with your parent about what they want. Make a list of their current medications. Find out who their primary care physician is and how to reach that office. Put together a folder, physical or digital, with the key documents: insurance cards, medication list, emergency contacts, and any legal documents that exist.
Then, if you want more structured guidance on navigating the system, building a proactive care plan, or understanding what resources are actually available in your area, that is what I do at Aging Together. I am most active on LinkedIn, and my website is aging-together.com.
And if you are a home health agency owner, a director of nursing, or someone building tools for home health, I would encourage you to remember that every patient your nurses visit has a family around them. They are part of the care team, whether or not they have been trained for it. The more prepared those families are, the better the outcomes for everyone.
Listen to the full conversation between Dr. Pooja Patel and Arvind Sarin on the Inside Home Health podcast series at copperdigital.com. To see how Copper Digital supports home health agencies with AI-assisted documentation and care coordination tools, request a demo. |
About the Author
Dr. Pooja Patel, OTR/L, BCGA, is an occupational therapist with board certification in gerontology and additional specialized training in dementia care and fall prevention. She has spent over a decade working within hospital systems, most recently focused on older adults and their family caregivers. She is the founder of Aging Together, a Chicago-based education and consulting practice dedicated to helping families navigate aging, caregiving, and the American care system proactively, before crisis forces the conversation. She can be reached at aging-together.com.
Related Reading

