Blog
Mar 17, 2026
The PDGM Comorbidity Adjustment: What Qualifies, What Gets Missed, and What It Costs

Arvind Sarin

Under the Patient-Driven Groupings Model, two factors determine most of your payment variation: the primary diagnosis clinical grouping and the comorbidity adjustment. Most agencies have done the work to understand primary diagnosis sequencing. Fewer have done the same work for comorbidity adjustment, and the gap shows up directly in revenue.
The comorbidity adjustment is not a supplemental correction to the base payment. It is a structured component of the PDGM HHRG calculation that can meaningfully increase the payment for medically complex patients. Those patients make up a large share of most home health caseloads. When their comorbidities are undercoded, the agency is not receiving the reimbursement the payment model was designed to provide. This post explains exactly how the comorbidity adjustment works, why qualifying conditions are consistently missed, and what has to change in the intake and coding workflow to capture it reliably. For the primary diagnosis side of the same problem, see our post on PDGM diagnosis sequencing.
How the PDGM Comorbidity Adjustment Works
PDGM assigns each 30-day payment period to a Home Health Resource Group based on five factors. The comorbidity adjustment is the third factor. It can take one of three values: no adjustment, a low comorbidity adjustment, or a high comorbidity adjustment. Each tier represents a different payment weight applied to the base HHRG payment.
The two-tier structure
Low comorbidity adjustment: applies when the patient has at least one qualifying comorbid condition coded as a secondary diagnosis on the claim. The qualifying conditions are defined by CMS in a specific comorbidity list that identifies conditions associated with significantly higher resource use in home health.
High comorbidity adjustment: applies when the patient has qualifying comorbid conditions from at least two different body system categories. This is the element most agencies miss. It is not simply about having two qualifying conditions. The conditions must fall into different body system categories as defined by CMS. A patient with three cardiovascular comorbidities may receive only the low adjustment because all three fall within the same body system category.
The payment difference between no adjustment and a high comorbidity adjustment is real and compounds across volume. A medically complex patient who qualifies for the high adjustment but is only receiving the low adjustment or no adjustment represents payment that the PDGM model was designed to provide and the agency is not capturing.
CMS updates the comorbidity list CMS publishes and periodically updates the list of qualifying comorbid conditions and the body system categories used for the high comorbidity adjustment. Agencies should verify that their coding teams are working from the current CMS comorbidity list, not a version from the initial PDGM implementation in 2020. The qualifying conditions and categories can change with each final rule update. |
What the Body System Category Requirement Actually Means
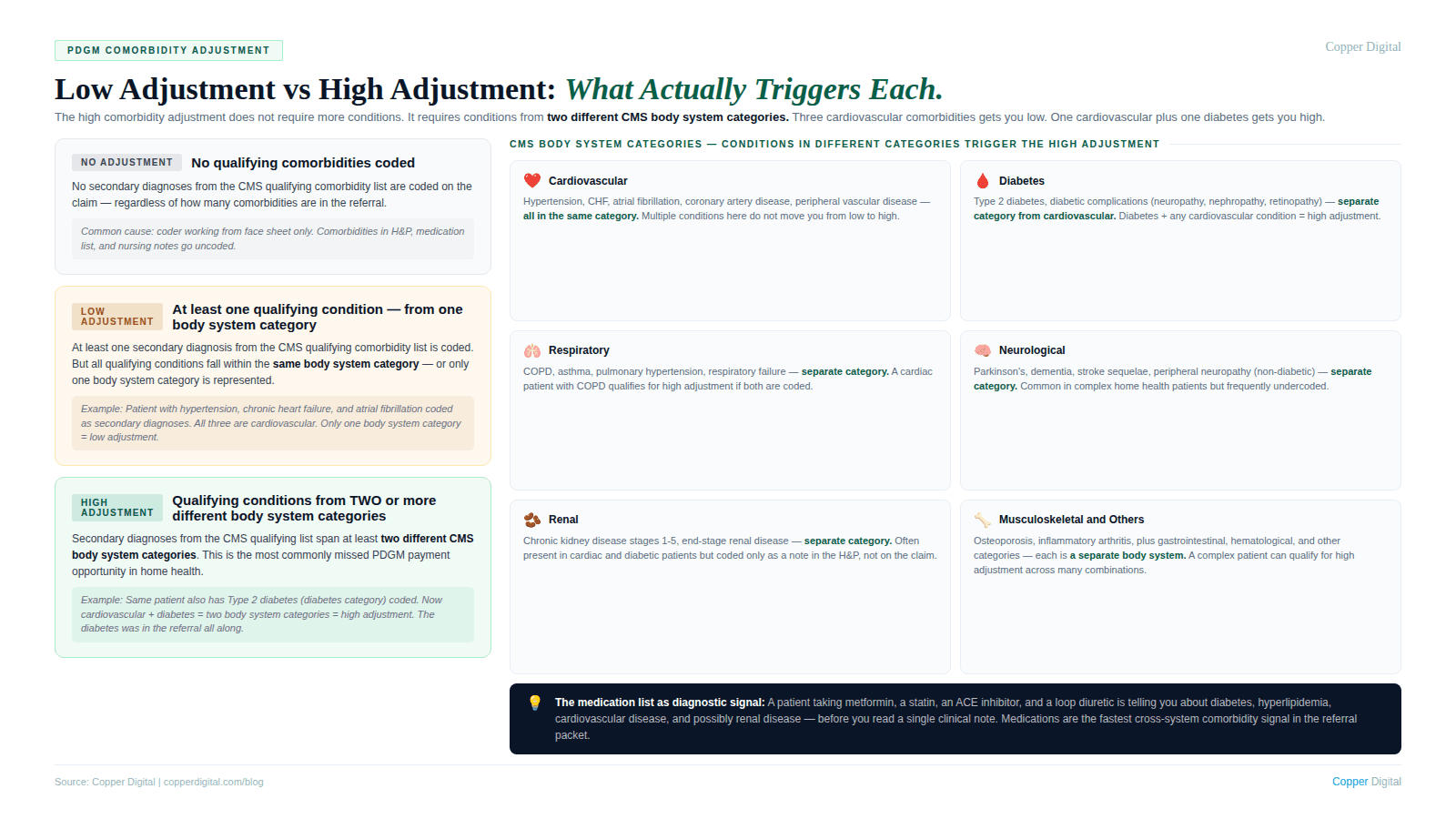
This is the most commonly misunderstood element of the comorbidity adjustment. The high adjustment does not require two qualifying conditions. It requires qualifying conditions from two different CMS-defined body system categories.
CMS organizes the qualifying comorbidity list by body system category: cardiovascular, diabetes, respiratory, neurological, renal, gastrointestinal, and others. For a patient to qualify for the high comorbidity adjustment, the coded secondary diagnoses must include at least one qualifying condition from two or more of these categories.
Why this creates systematic underpayment
A patient with hypertension, chronic heart failure, and atrial fibrillation has three qualifying cardiovascular comorbidities. If only these three are coded, the patient receives the low comorbidity adjustment, not the high adjustment, because all three conditions fall within the same body system category.
That same patient, if they also have type 2 diabetes, now qualifies for the high comorbidity adjustment because diabetes falls in the diabetes body system category, separate from the cardiovascular category. If the diabetes is documented in the referral but not coded as a secondary diagnosis, the agency receives the low adjustment when the high adjustment was appropriate.
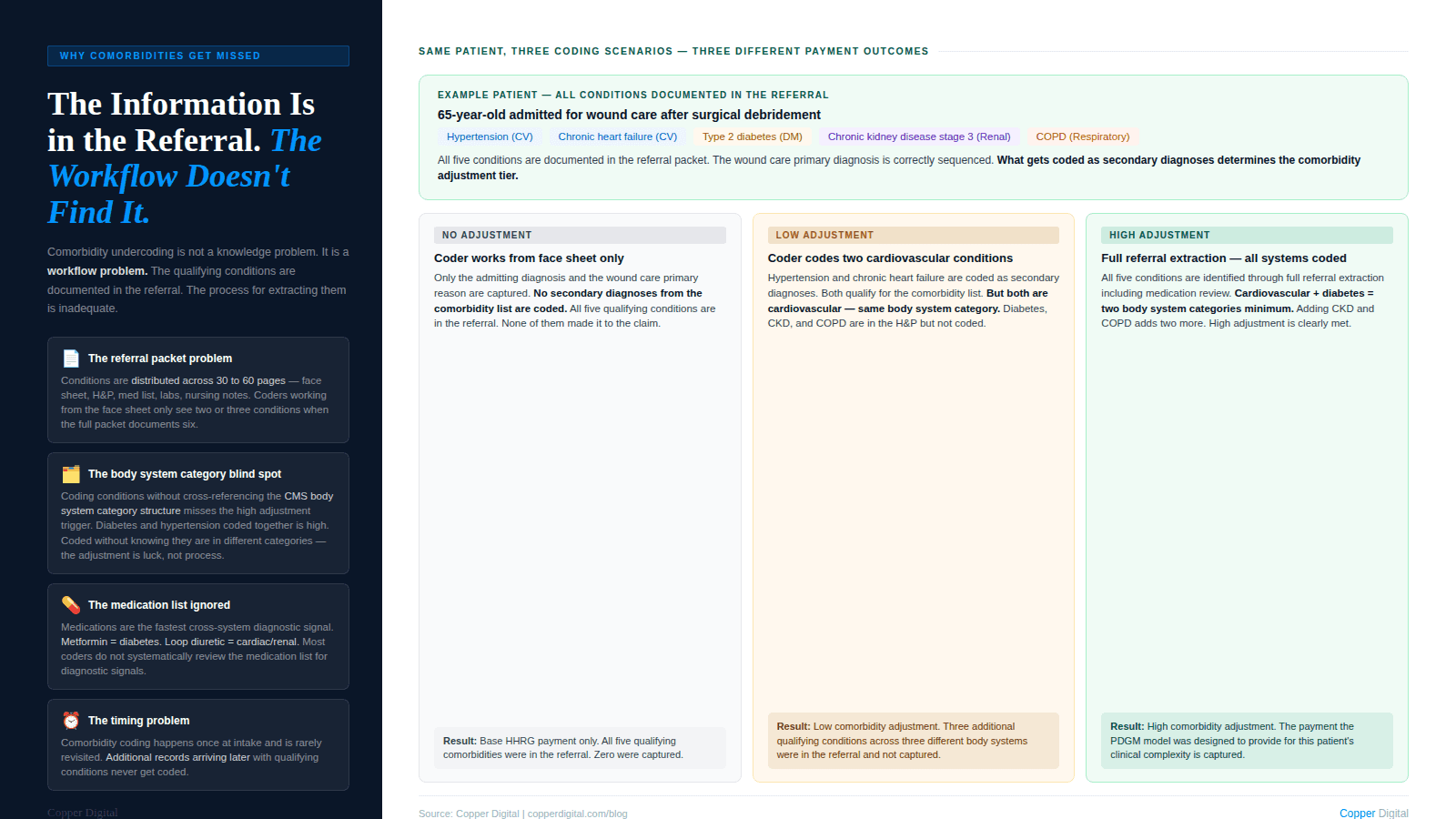
This pattern plays out across thousands of claims at agencies with medically complex caseloads. The information to support the high adjustment is almost always in the referral documentation. The question is whether the coding workflow extracts it.
The qualifying comorbidities are in the referral. The question is whether the workflow gets them out. A patient with hypertension, heart failure, and diabetes documented in a 40-page discharge packet may be coded with only two of those three conditions if the coder is working from the face sheet rather than the full clinical record. |
Why Qualifying Comorbidities Are Consistently Missed
The referral packet problem
Home health referrals arrive as multi-page documents. A medically complex patient discharged from an acute care setting can generate a referral packet of 30 to 60 pages including physician orders, discharge summaries, medication reconciliation lists, lab results, imaging reports, and nursing notes. The comorbid conditions that would qualify for the high comorbidity adjustment are distributed across these documents. The admitting diagnosis appears on the face sheet. The diabetes appears in the H&P. The chronic kidney disease appears in the lab results. The neuropathy appears in the nursing notes. If the coder is working from the face sheet, they code two conditions. If they work from the full packet, they may code five or six. This is the same referral extraction problem that drives primary diagnosis sequencing errors. The comorbidity adjustment failure is a downstream consequence of the same root cause.
The body system category blind spot
Even coders who are working from complete referral information often miss the high comorbidity adjustment because they are coding conditions without cross-referencing against the CMS body system category structure. Coding diabetes and hypertension as secondary diagnoses is accurate ICD-10 coding. Knowing that those two conditions fall into different body system categories and therefore trigger the high comorbidity adjustment requires an additional layer of PDGM-specific knowledge that not all coding staff have internalized.
The specificity gap
Like primary diagnosis coding, comorbidity coding is subject to ICD-10 specificity requirements. A patient with diabetic peripheral neuropathy coded as unspecified diabetes (E11.9) rather than type 2 diabetes with diabetic peripheral neuropathy (E11.40) may have a secondary diagnosis that still qualifies for the comorbidity adjustment, but is coded at a lower specificity than the documented clinical picture supports. Coding to the highest available specificity is a standard requirement, but comorbidity codes in the context of PDGM have additional significance because the specific code may determine which body system category the condition falls into.
The timing problem
Comorbidity coding happens at intake, before the start of care visit. The referral documentation available at intake may not be complete. Additional clinical information may arrive with the face-to-face documentation, the physician H&P, or records from other treating providers. If comorbidity coding is done once at intake and never revisited as additional information arrives, qualifying conditions that appear later in the record may never be coded.
What a Systematic Comorbidity Review Looks Like
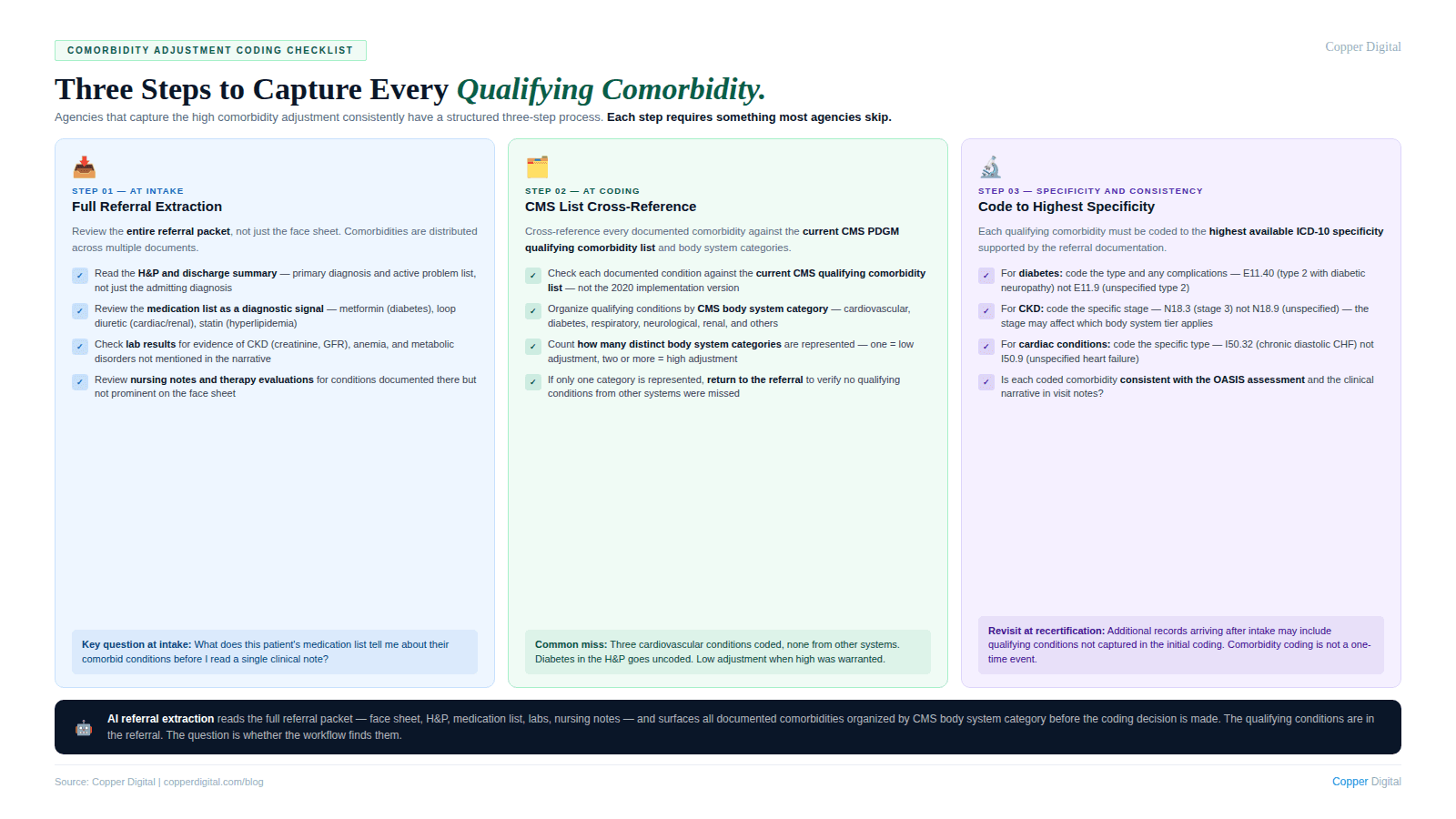
Agencies that capture comorbidity adjustment revenue consistently have a structured process for comorbidity identification that goes beyond the face sheet. The process has three components.
Full referral extraction at intake
Every section of the referral packet should be reviewed for qualifying comorbidities, not just the face sheet and the primary diagnosis section. The medication list is particularly valuable: a patient taking metformin, a statin, an ACE inhibitor, and a loop diuretic is telling you about diabetes, hyperlipidemia, cardiovascular disease, and potentially renal insufficiency before you have read a single clinical note. Medications are a systematic signal of underlying conditions that may qualify for the comorbidity adjustment.
Cross-reference against the CMS comorbidity list and body system categories
After extracting all documented comorbidities from the referral, each condition should be cross-referenced against the current CMS PDGM comorbidity list to determine which qualify and which body system categories they represent. This cross-reference is a mechanical process that can be systematized. It does not require clinical judgment. It requires a current copy of the CMS comorbidity list and a structured process for checking each documented condition against it.
Coding to the highest available specificity
Each qualifying comorbidity should be coded to the highest ICD-10 specificity level supported by the referral documentation. This means coding laterality, etiology, stage, and anatomical location where available. For conditions like diabetic complications, peripheral vascular disease, and chronic kidney disease, the specific code determines the clinical accuracy of the claim and may affect which body system category the condition falls into.
The Revenue Impact of Getting This Right
The PDGM comorbidity adjustment affects every 30-day payment period for patients whose comorbid conditions qualify. The payment differential between adjustment tiers is meaningful on a per-episode basis and compounds significantly at the volume of a mid-sized or large home health agency.
A patient who qualifies for the high comorbidity adjustment but is receiving the low adjustment due to incomplete secondary diagnosis coding is generating less revenue than the PDGM model intends for their level of clinical complexity. Across a caseload where a significant proportion of patients have multi-system comorbidities, systematic undercoding of the comorbidity adjustment represents a material revenue shortfall.
The important distinction here is that this is not upcoding. It is not coding conditions that are not documented. It is coding to what is documented in the referral, at the appropriate specificity, and cross-referencing against the PDGM comorbidity criteria. The payment the agency is not receiving was designed into the PDGM model specifically to compensate for the higher resource use of patients with multiple comorbidities. Failing to capture it does not protect the agency from anything. It simply leaves money on the table.
How AI-Assisted Intake Changes the Comorbidity Equation
The comorbidity adjustment problem is a structured information extraction problem. The qualifying conditions are in the referral documentation. The question is whether the workflow gets them out consistently. AI tools trained on clinical documentation can extract diagnoses, comorbidities, and medication information from referral packets and organize them into a structured summary. When that summary is cross-referenced against the PDGM comorbidity list and body system category structure, the result is a systematic comorbidity identification process that does not depend on a coder having time to read a 60-page packet or remembering to check the medication list for diagnostic signals.
This is the same referral extraction capability that addresses primary diagnosis sequencing accuracy and denial prevention. The clinical information in the referral serves multiple downstream purposes. Extracting it completely and accurately at intake produces better primary diagnosis coding, better comorbidity adjustment capture, and better start of care documentation quality simultaneously.
Comorbidity Adjustment Coding Checklist
Use this checklist at intake and at coding to verify that the comorbidity adjustment is being captured accurately for each patient.
At intake
Has the full referral packet been reviewed for comorbidities, not just the face sheet and primary diagnosis section?
Has the medication list been reviewed as a signal of undocumented comorbidities?
Have lab results been reviewed for evidence of conditions such as chronic kidney disease, anemia, or metabolic disorders that may not appear prominently in the clinical narrative?
At coding
Has each documented comorbidity been cross-referenced against the current CMS PDGM comorbidity qualifying list?
Have the qualifying comorbidities been organized by CMS body system category to determine whether the high comorbidity adjustment threshold is met?
Is each qualifying comorbidity coded to the highest available ICD-10 specificity supported by the referral documentation?
If the patient qualifies for the low adjustment, are there additional body system categories represented in the clinical record that could qualify for the high adjustment if coded?
Consistency check
Is the overall secondary diagnosis coding consistent with the clinical picture described in the OASIS assessment and the visit notes? See PDGM diagnosis sequencing for the primary diagnosis side of the same consistency requirement.
Has additional documentation arrived since intake that may include qualifying comorbidities not captured in the initial coding?
Copper Digital extracts diagnosis and comorbidity information from the full referral packet at intake, cross-references qualifying conditions against the PDGM comorbidity list and body system categories, and surfaces the high comorbidity adjustment opportunity before the coding decision is made. Request a demo to see how this works in your agency's intake workflow. |
Related Reading

