Blog
Mar 9, 2026
Your EMR Was Not Built for Your Nurses

Gaurav Henry

I have been having a version of the same conversation with home health leaders for the past three years. A DON tells me their nurses are exhausted. OASIS accuracy is inconsistent. The QA queue never clears. They have tried training, incentives, and staffing up. Nothing moves the needle. When I ask them to describe what their nurses actually do during a Start of Care visit, the story is always the same: the nurse walks in, opens the EMR, and begins answering questions in the order the system presents them. On and on through a form designed around regulatory requirements, not around how a clinician thinks.
I recently sat down with Kathy Duckett to dig into why. Kathy has spent decades at the intersection of nursing practice and technology, advising agencies, vendors, and national organizations. Her session at the NARC conference, Next-Gen Home Health EMR: Nursing Expertise Plus AI, reframed something the industry has been getting wrong for a long time. Here is what I took from that conversation.
EMRs Were Designed Around OASIS, Not Around Nurses
When you ask a nurse to fill out a form in a fixed sequence, you are not asking her to assess a patient. Nurses are trained to assess holistically. You walk in, observe the patient, and based on what you find, the assessment branches organically. The assessment follows the patient, not a form.
But EMRs are linear because the underlying OASIS instrument is linear, and the OASIS is linear because CMS specifies the questions in a fixed order. There is no flexibility to reframe a question, reorder the assessment, or let the clinical picture guide what gets documented when. So nurses work around the conflict: they answer the question on screen before they have the information to answer it accurately, come back to revise, and toggle between sections trying to reconcile entries made at different points in the visit. That friction is not a training problem. It is a design problem.
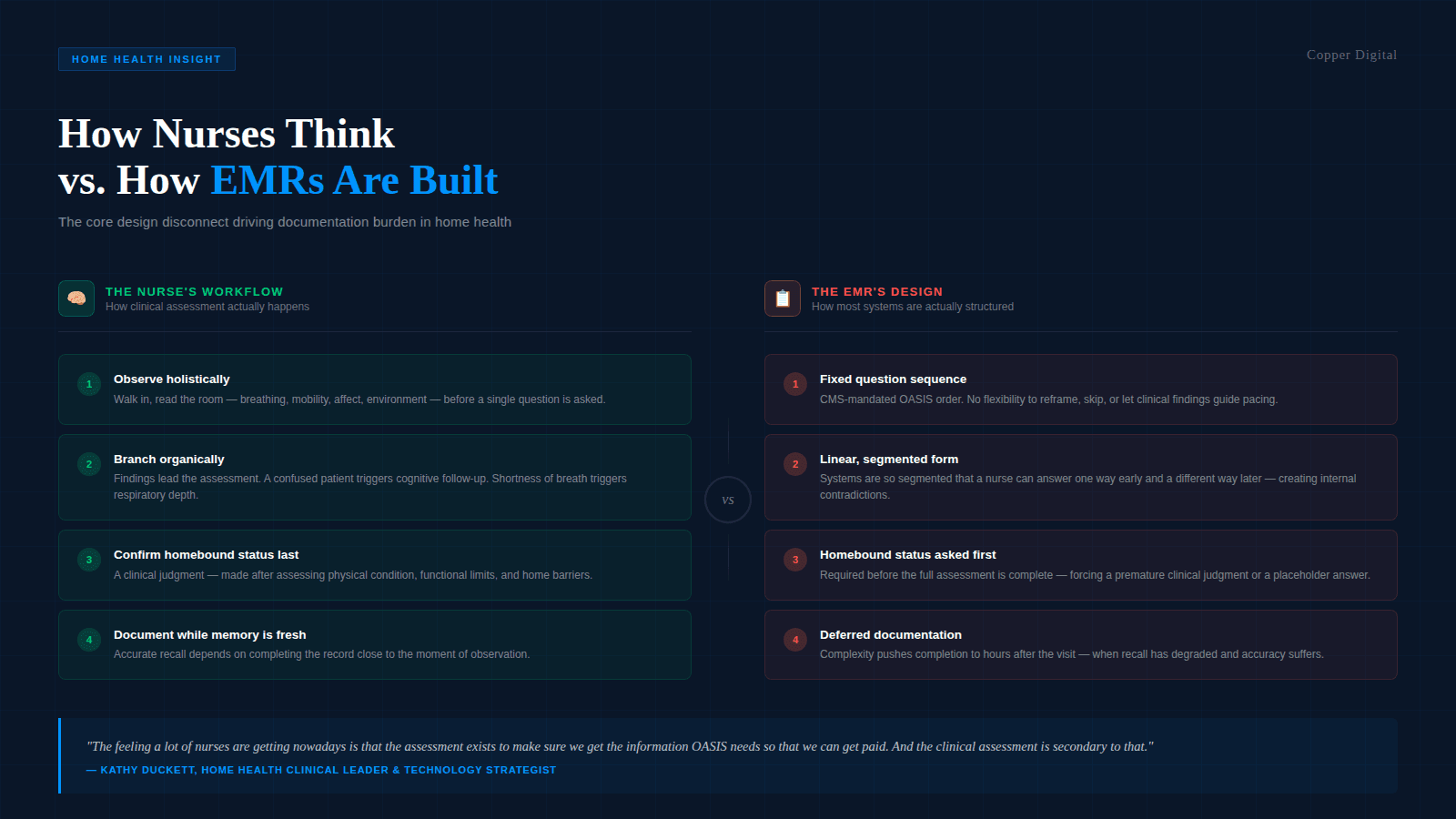
The feeling a lot of nurses are getting nowadays is that the assessment exists to make sure we get the information OASIS needs so that we can get paid. And the clinical assessment is secondary to that. |
The Homebound Status Problem
Kathy gave one example that illustrates the design flaw precisely. For a patient to qualify for home health under Medicare, they have to meet the homebound criterion. So most EMRs ask the nurse to confirm homebound status early in the assessment flow. Logically, if the patient is not homebound, there is no point in completing a two-hour assessment.
The problem: homebound status is a clinical judgment based on physical condition, functional limitations, and the barriers that make leaving the home taxing or unsafe. You cannot make that call when you walk through the door. Kathy's framing was direct: "The homebound status I pick when I first walk in may be different once I've completed the entire assessment. There may be a more compelling reason why the patient is homebound than was first obvious."
So the nurse enters a placeholder that may be wrong, or delays answering, and gets flagged for an incomplete form. Either way, the documentation does not reflect the actual clinical reasoning. This is what we mean when we talk about the clinical story not making sense. The contradictions auditors flag often trace back not to clinician error but to a workflow that forced documentation decisions before the information was available to make them.
The 20 Percent Memory Problem
Kathy referenced studies on clinical memory that should concern every agency owner: the farther away you get from the moment of assessment, the less you remember. If a nurse sees a patient at eight in the morning and does not finish her documentation until four or five in the afternoon, she is working from roughly 20 percent of what she actually observed.
If you see a patient at 8 a.m., by the time you're getting to your documentation, which could be four or five or six hours later, you probably remember about 20 percent of that interaction. |
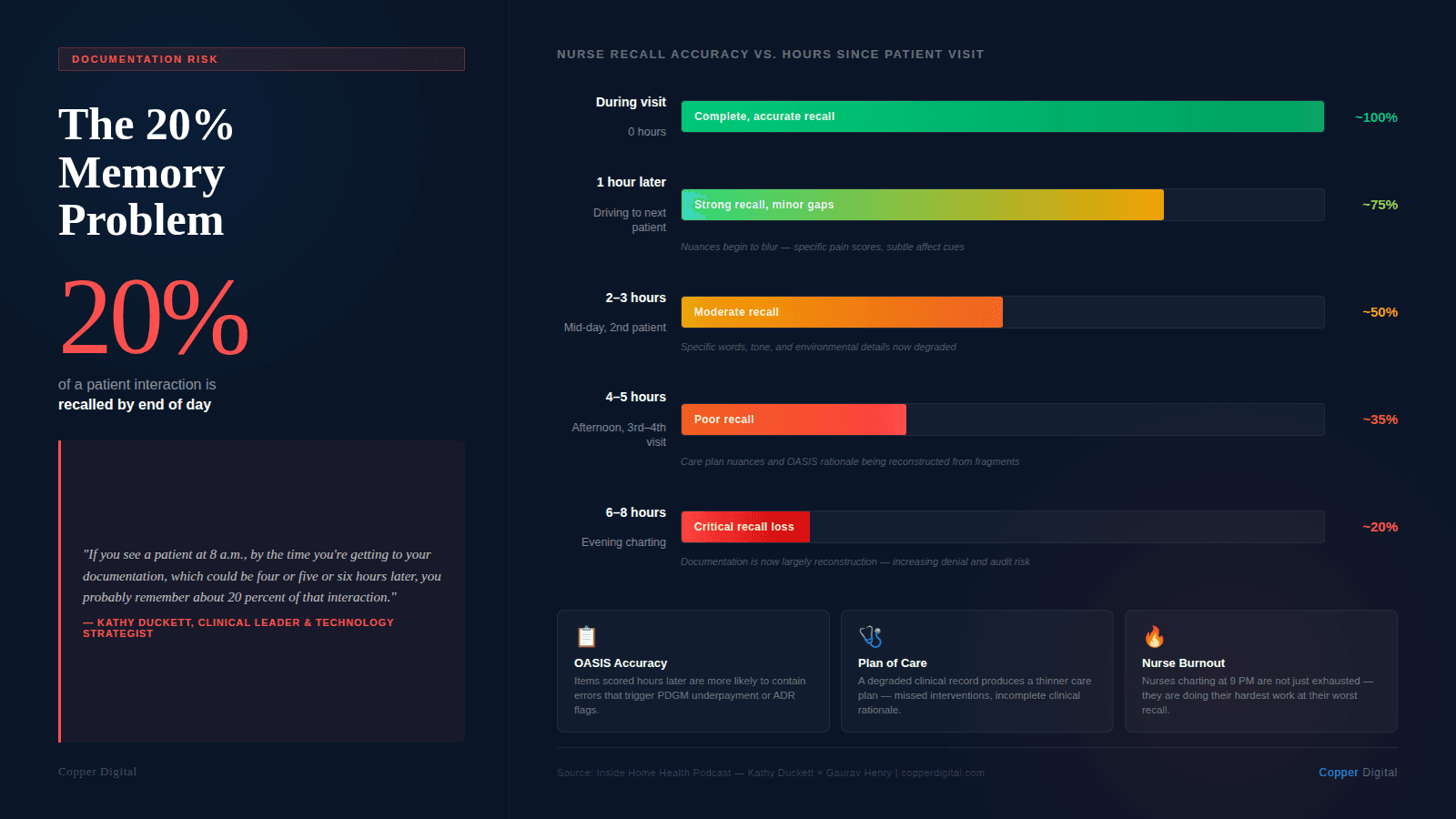
This is the hidden cost of documentation overload that leaders consistently underestimate. They see nurse exhaustion, turnover, QA errors. But they do not always connect those back to the fact that the documentation workflow forces nurses to work from degraded memory. A degraded clinical record affects the plan of care, which affects outcomes, which affects your HHVBP score.
Compliance-First Design Loses the Patient
Kathy was careful to say compliance matters. OASIS data drives quality measurement, reimbursement, and public reporting. Getting it right is not optional. But there is a difference between designing a tool that helps a nurse be compliant while delivering care, and designing a tool where compliance fields come first, and clinical reasoning works around them.
When the system is built the wrong way around, you get charts that are technically complete and clinically thin. The OASIS fields are populated, but the nuances that would inform a genuinely individualized care plan are not there. Not because the nurse did not observe them, but because the system did not make space for them. As Kathy put it: "If I'm just being compliant, answering A through G, but not using the critical thinking nurses are educated to do, then I'm filling out the paperwork, but I'm not necessarily taking care of the patient. And you have to do both."
What a Dynamic Record Would Look Like
When I asked Kathy what a nurse-centered EMR would actually look like in practice, she was not describing features. She was describing a workflow. A dynamic record would update in real time as the nurse completes her assessment. It would prompt when something appears to be missing during the visit, not after it. As interventions are documented, the care plan would update automatically. By discharge, the care plan would be a living record of what happened, not a form reconstructed from memory.
She also described the pre-visit briefing: before walking in, the nurse should receive a short synthesis of what happened on the last visit, what the current plan intended, and what has changed since, including labs, therapy visits, and any physician contact. AI can produce that. That is exactly what pre-visit automation should do, not replace the nurse's judgment, but make sure the clinical story is coherent before she walks through the door, not reconstructed afterwards.
The Nurse Involvement Problem
The part of our conversation that will resonate most with clinical leaders: vendors involve nurses late, if at all. And when they do, the assumption is that a nurse is a nurse. A hospital nurse, an ICU nurse, and a home health nurse are all interchangeable. Kathy's analogy was sharp: that is like saying a corporate lawyer can walk into family court tomorrow because they both went to law school.
Home health nursing is a specialty. The assessment happens alone in a patient's home, without backup, often with five more patients on the schedule. The clinical judgment required is different from acute care. A tool designed for that environment cannot be designed by someone who has never worked in it.
The pattern Kathy described is painfully familiar. Vendors go to the CEO, do a demo, and the purchase is approved based on what leadership saw in a conference room. Field nurses are then expected to adapt their workflows around a system that was never designed around them. Productivity drops. Nurses struggle. The CEO is frustrated. The vendor says it worked fine in the demo.
What meaningful involvement actually looks like
Before any EMR purchase, field nurses should be involved as testers, not observers. Not the DON who has not done a SOC visit in a decade. The nurse who did three admissions last week. Kathy told a story about a healthcare system that got this right: when their EMR did not integrate with their telemedicine program, they insisted the vendor send a technical team to work directly with clinical staff. The program launched with what it needed, and it worked. That is not common. But it is what we should be demanding.
What Leaders Should Do Now
I left the conversation with Kathy with three things I want to say directly to agency owners and directors.
If your nurses are frustrated with your EMR, that frustration is clinically grounded. They are not resistant to change. They are struggling because the system was not designed around how they think. That distinction matters for how you respond to it.
Documentation burden is not just an HR problem. Every hour a nurse spends reconstructing visit notes from memory is an hour where the clinical record degrades. That affects care plans, continuity, OASIS accuracy, and audit exposure.
Involve field nurses before you sign anything. Not after. Let them use the tool. Let them tell you where it breaks. A tool the CEO loves, and the field nurse cannot use, is not a tool. It is an expensive problem waiting to happen.
The frustration nurses feel today is not about technology. It is about being treated as data entry operators rather than clinical professionals. When your EMR asks a nurse to confirm homebound status before she has assessed the patient, it communicates something about how the system views her role. The technology we build communicates the same thing. Either we build tools that support nursing judgment, or we build tools that work around it. Nurses know the difference.
Listen to the full conversation with Kathy Duckett on the Inside Home Health podcast series at our YouTube channel. To see how Copper Digital approaches pre-visit automation and OASIS documentation support, request a demo. |
About the Author
Gaurav Henry is Chief Marketing Officer of Copper Digital, a home health automation company building AI agents that reduce documentation burden, improve OASIS accuracy, and give clinicians time back. He hosts the Inside Home Health podcast series alongside Arvind Sarin.
Related Reading
An Autopsy of a Start of Care: The 2-Hour Visit That Takes 6 Hours
How Medicare Bots Find the Errors Humans Miss in OASIS Documents
Why Home Health Documentation Is Driving Your Best Nurses Out the Door

