Blog
Mar 4, 2026
PDGM Diagnosis Sequencing: The Coding Decision That Determines Your Reimbursement

Arvind Sarin

The patient has been admitted. The OASIS is complete. The plan of care is drafted. And somewhere in the referral packet, buried in a 40-page hospital discharge summary, is the clinical information that will determine how much your agency gets paid for this entire episode.
Under the Patient-Driven Groupings Model, the primary diagnosis you select at start of care is not a formality. It is the single most consequential coding decision in home health billing. Get it right and your payment accurately reflects the patient's clinical complexity. Get it wrong and you are either leaving legitimate reimbursement uncollected or creating audit exposure that surfaces months later as a denial you have to fight through the appeals process.
This post explains how PDGM diagnosis sequencing actually works, why it fails consistently in practice, and what has to change upstream to get it right.
How PDGM Actually Determines Your Payment
PDGM replaced the old visit-based payment system in January 2020. Under the previous system, payment was tied primarily to therapy visit thresholds. Under PDGM, payment is determined at the start of each 30-day payment period by a set of patient characteristics captured at the time of admission. The primary diagnosis is the first and most influential of those characteristics.
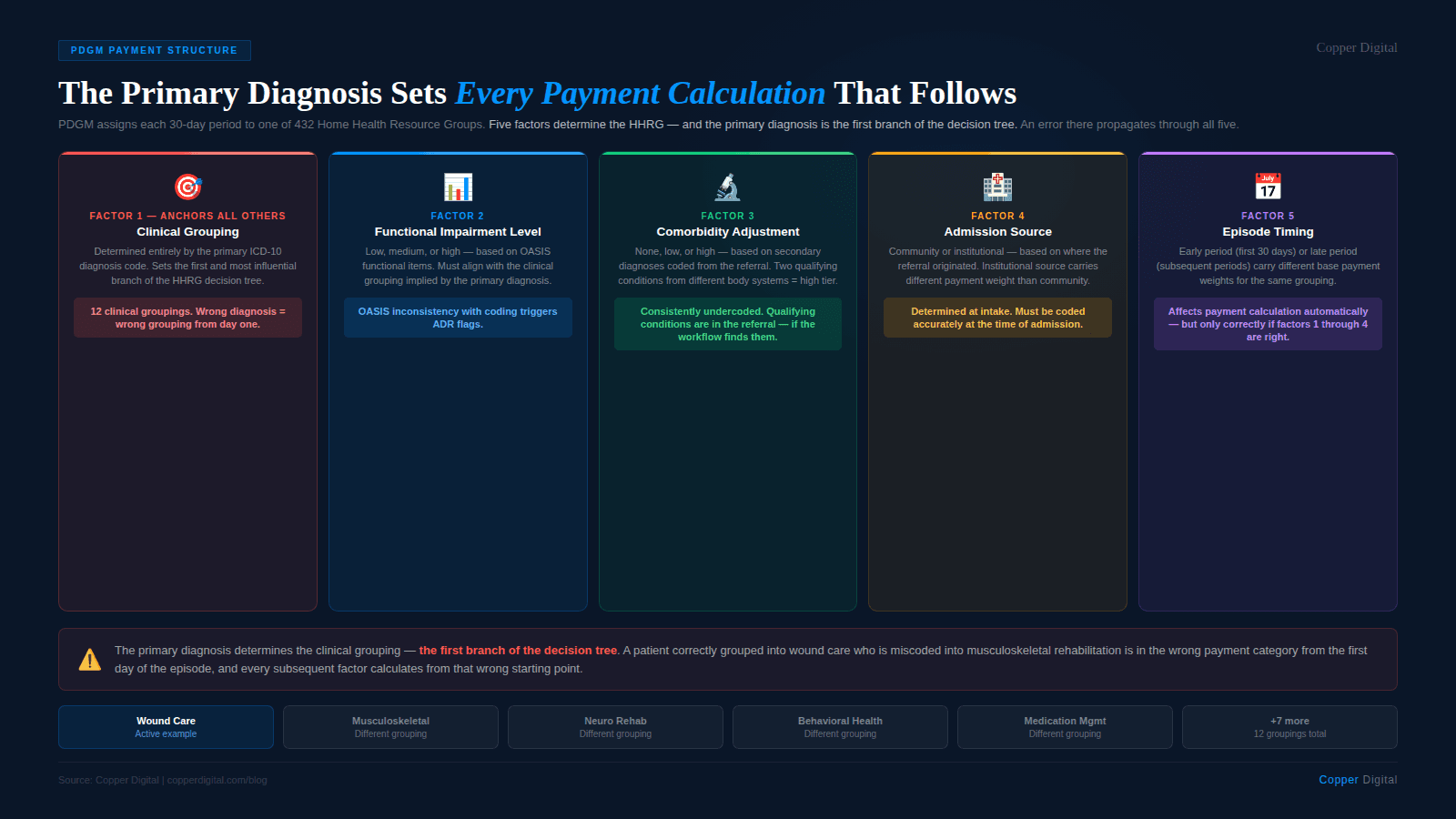
Each 30-day payment period is assigned to one of 432 Home Health Resource Groups. The HHRG determines the base payment rate for that period. The HHRG assignment flows from a five-factor calculation:
Clinical grouping — determined entirely by the primary diagnosis ICD-10 code
Functional impairment level — low, medium, or high, based on OASIS functional items
Comorbidity adjustment — none, low, or high, based on secondary diagnoses
Admission source — community or institutional, based on where the referral originated
Early versus late episode — first 30-day period versus subsequent periods carry different weights
The primary diagnosis determines the clinical grouping, and the clinical grouping is the anchor of the entire payment calculation. There are twelve clinical groupings under PDGM, and the payment differences between them are substantial. Musculoskeletal rehabilitation is grouped differently from wound care. Behavioral health is grouped differently from neuro rehabilitation. Medication management is grouped differently from complex nursing interventions. Selecting the wrong primary diagnosis does not just affect the label on the claim. It routes the entire episode into a different payment category.
The 432 HHRG structure PDGM has 432 possible Home Health Resource Groups. The primary diagnosis drives the clinical grouping component, which is one of five factors. But because the clinical grouping is the first branch of the decision tree, an error there propagates through every subsequent calculation. A patient correctly grouped into wound care who is miscoded into musculoskeletal rehabilitation is in the wrong branch of the tree from the first day of the episode. |
What Primary Diagnosis Sequencing Actually Means
Diagnosis sequencing is the process of determining which ICD-10 code to list first on the claim. Under PDGM, the primary diagnosis must be the condition that is the primary reason for home health services during the episode. It cannot be a symptom when the underlying condition is known. It cannot be a historical diagnosis that is no longer the reason for current treatment. It cannot be a comorbidity that is being managed but is not the focus of skilled care.
CMS has specific sequencing conventions that apply to home health coding, which differ in important ways from inpatient coding conventions. Home health agencies that use coders trained primarily in hospital billing often apply inpatient sequencing logic to home health claims, which produces coding that is technically formatted but clinically misaligned with PDGM grouping categories.
What the primary diagnosis must be
The primary diagnosis must describe why the patient needs home health at this specific point in time. If the patient is recovering from a hip replacement, the primary diagnosis should reflect the orthopedic condition and the current focus of rehabilitation, not the surgical history code. If the patient has chronic heart failure and was discharged after an exacerbation, the primary diagnosis should reflect the active clinical focus, whether that is the CHF management, associated wound care, or a specific complication, depending on what is actually driving the skilled nursing visits.
The primary diagnosis also cannot be a code that is on CMS's list of diagnoses that are not acceptable as primary for home health. These include symptoms, signs, and abnormal clinical findings when the underlying condition is known, certain injury sequelae codes used incorrectly, and codes from categories that CMS has excluded from primary diagnosis use in home health.
What sequencing errors actually look like
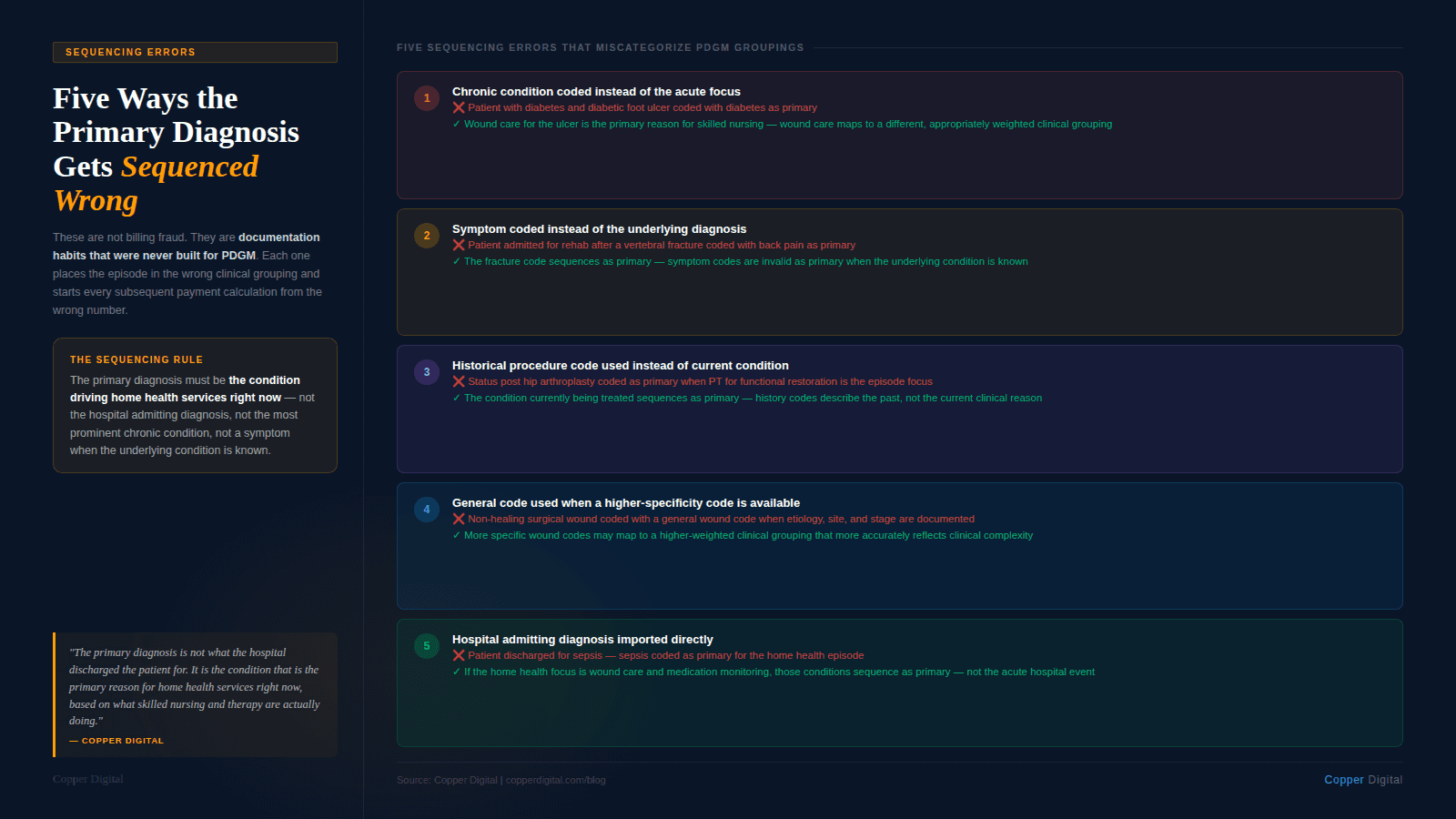
The most common sequencing errors in home health fall into five patterns:
Using the chronic condition instead of the acute focus. A patient with diabetes and a diabetic foot ulcer is coded with diabetes as primary when wound care for the ulcer is the primary reason for skilled nursing. The wound care clinical grouping and the diabetes clinical grouping carry different payment weights.
Using the symptom instead of the diagnosis. A patient admitted for pain management and rehabilitation after a vertebral fracture is coded with back pain as the primary diagnosis instead of the fracture code. This places the episode in the wrong clinical grouping and may trigger a coding edit flag.
Using the historical procedure code instead of the current condition. A patient is coded with a status post hip arthroplasty code when the current clinical focus is physical therapy for functional restoration. The sequencing should lead with the condition being treated, not the historical procedure.
Missing a higher-specificity code. A patient with a non-healing surgical wound is coded with a general wound care code when a more specific wound etiology code exists and would more accurately reflect the clinical complexity. The more specific code may map to a different, more appropriate clinical grouping.
Using the admitting diagnosis from the hospital rather than the home health primary reason. The hospital discharged the patient for sepsis. The home health episode is primarily for wound care management and medication monitoring. Using the sepsis code as the home health primary diagnosis misrepresents the focus of home health services and may place the episode in an inappropriate grouping.
The primary diagnosis is not what the hospital discharged the patient for. It is the condition that is the primary reason for home health services right now, at the start of this episode, based on what skilled nursing and therapy are actually doing. |
Why Sequencing Errors Happen Consistently
If the rules are documented and available, why do sequencing errors remain so common? The answer is not a lack of will to get it right. It is a structural problem in how clinical information moves from the referral source to the coder.
The referral packet problem
Home health agencies typically receive referrals as fax transmissions or electronic document packets. A referral for a medically complex patient can easily run 30 to 60 pages: physician orders, hospital discharge summaries, medication reconciliation lists, lab results, imaging reports, therapy evaluations, and nursing notes from the inpatient stay.
The nurse conducting the start of care visit may have access to this packet, but she is focused on the clinical assessment, not the coding determination. The coder who will assign the primary diagnosis may be working from a subset of the referral documentation, or from a face sheet that summarizes the patient's conditions without fully capturing the clinical picture. The pre-visit briefing gap that affects clinical documentation quality also affects coding quality: when the full referral is not synthesized into usable clinical context before the episode begins, both the OASIS and the coding start from an incomplete picture.
The OASIS and coding disconnect
Under PDGM, the OASIS functional assessment and the ICD-10 diagnosis coding should tell a consistent clinical story. A patient coded into the wound care clinical grouping should have OASIS items that reflect wound-related functional limitations and care needs. A patient coded into musculoskeletal rehabilitation should have OASIS functional status items that align with rehabilitation goals.
When coding is done in isolation from the OASIS assessment, these alignments break down. The coder assigns a primary diagnosis based on the referral documents. The clinician completes the OASIS based on the clinical assessment. If these two processes are not coordinated, the result is a chart where the diagnosis grouping and the functional status documentation point in different directions. This is exactly the type of internal inconsistency that triggers ADR review flags.
The specificity problem
ICD-10 is a highly granular coding system with over 70,000 codes. For many conditions, there are multiple codes available at different levels of specificity, and the more specific codes may map to different PDGM clinical groupings than the general codes. A coder who defaults to a general code when a more specific one exists is not necessarily making an error under ICD-10 conventions, but may be leaving the episode in a lower-weighted clinical grouping when a more specific code would more accurately reflect the patient's condition and receive appropriate PDGM weighting.
This is particularly relevant for wound care, which has extensive ICD-10 specificity requirements for wound etiology, anatomical location, laterality, and healing stage. An agency that consistently uses unspecified wound codes when more specific codes are available and clinically supportable is systematically undercoding wound complexity.
The Comorbidity Layer: Secondary Diagnoses That Change the Payment
PDGM's comorbidity adjustment is a separate payment factor from the clinical grouping, but it is also driven by diagnosis coding and is consistently undercoded. The comorbidity adjustment can increase the base payment by a meaningful percentage, but only if the relevant secondary diagnoses are coded and documented.
Under PDGM, the comorbidity adjustment has two tiers. A low comorbidity adjustment applies when the patient has at least one qualifying comorbid condition from a defined list. A high comorbidity adjustment applies when the patient has at least two qualifying comorbid conditions from two different body system categories. The adjustment is calculated based on what is coded on the claim, not what is in the patient's medical history.
The clinical information to support a high comorbidity adjustment is almost always present in the referral documentation. Patients admitted to home health are typically medically complex, with multiple chronic conditions. A patient admitted primarily for wound care may have diabetes, hypertension, chronic kidney disease, and peripheral neuropathy all documented in the hospital records. Each of these may qualify as a comorbidity under PDGM. If only two of the four are coded as secondary diagnoses, the comorbidity tier calculation may be lower than the patient's clinical complexity warrants.
The comorbidity adjustment in practice The specific conditions that qualify for the PDGM comorbidity adjustment, and which body system categories they fall into, are defined by CMS and updated periodically. The high comorbidity adjustment requires conditions from two different body system categories. This means a patient with multiple cardiovascular conditions may only receive the low adjustment even if multiple cardiovascular comorbidities are coded, because they are all in the same body system. Understanding which conditions trigger which tiers, and coding all eligible conditions from the referral documentation, requires clinical coding expertise that many home health agencies do not have in-house. |
What Correct Sequencing Requires in Practice
Getting PDGM diagnosis sequencing right consistently is not primarily a knowledge problem. Most home health billing and coding professionals understand the rules. It is a workflow problem. The clinical information needed to make the correct sequencing decision is often not in the right format, in the right hands, at the right time.
Correct sequencing in practice requires three things to happen well:
1. Full referral extraction before coding begins
The primary diagnosis selection should be informed by the complete clinical picture from the referral, not just the face sheet or the admitting diagnosis. This means someone, whether a coder, a clinical supervisor, or an AI-assisted workflow, needs to review the full referral documentation and identify the clinical findings that are most relevant to the home health episode before the primary diagnosis is selected.
For agencies receiving high referral volumes, this is not realistically achievable through manual review at scale. A 60-page hospital discharge packet reviewed under time pressure at admission produces a different coding outcome than the same packet reviewed systematically with the relevant clinical details extracted and surfaced.
2. Alignment between OASIS assessment and diagnosis coding
The OASIS functional assessment and the ICD-10 coding should be reviewed together before the claim is submitted. The clinical grouping implied by the primary diagnosis should be consistent with the OASIS items that reflect the patient's functional status and care needs. When these are reviewed in isolation, misalignments that create both reimbursement errors and audit risk go undetected.
3. Systematic secondary diagnosis extraction
The comorbidity adjustment depends on coding all qualifying secondary diagnoses from the referral documentation. This requires a systematic process for extracting secondary diagnoses from the full referral packet, verifying that each is documented and clinically relevant to the current episode, and coding to the highest available specificity. Without a systematic process, secondary diagnosis coding defaults to whatever conditions are most prominent in the summary documents, which is typically a fraction of what is actually documented in the full clinical record. This connects directly to the documentation accuracy and OASIS completeness work that shapes the clinical record from the start of care.
How AI-Assisted Documentation Changes the Sequencing Equation
The PDGM coding problem is a structured information extraction problem. The information needed to make the correct primary diagnosis selection and identify all qualifying secondary diagnoses is in the referral documentation. The challenge is getting it out of a 60-page mixed-format document and into the hands of the person making the coding decision, accurately and consistently, at the volume that home health operations require.
AI-assisted clinical documentation workflows address this at the point where the problem originates: the referral intake.
Referral document extraction
AI tools trained on clinical documentation can extract diagnosis codes, comorbidities, active conditions, medication lists, and clinical narrative from referral packets and organize them into a structured clinical summary. This gives the coding team a synthesized view of the patient's clinical picture rather than a 60-page document that requires manual reading. The extracted information can be presented in a format that directly informs the primary diagnosis selection decision: what conditions are present, which are the focus of active treatment, and which qualify for PDGM comorbidity adjustment.
Primary diagnosis validation
Before a claim is submitted, an AI-assisted validation check can flag situations where the selected primary diagnosis appears inconsistent with the OASIS assessment or the clinical narrative. If the primary diagnosis maps to a wound care grouping but the OASIS does not document wound-related functional limitations, that inconsistency surfaces before submission rather than during an ADR review. If the primary diagnosis is a symptom code when the underlying condition is documented in the referral, that flags as a potential sequencing error that warrants review.
Secondary diagnosis optimization
AI extraction of secondary diagnoses from the full referral documentation,cross-referenced against the PDGM comorbidity adjustment criteria, can surface qualifying conditions that would be missed in a manual review. This is not upcoding. It is coding to what is actually documented. The conditions are in the referral. The question is whether the workflow extracts them consistently or inconsistently, and that question has a direct payment consequence.
PDGM coding accuracy is a structured information extraction problem. The clinical information needed to sequence correctly is in the referral. The question is whether the workflow gets it out consistently and puts it in the hands of the person who needs it, before the coding decision is made. |
A PDGM Diagnosis Sequencing Review Checklist
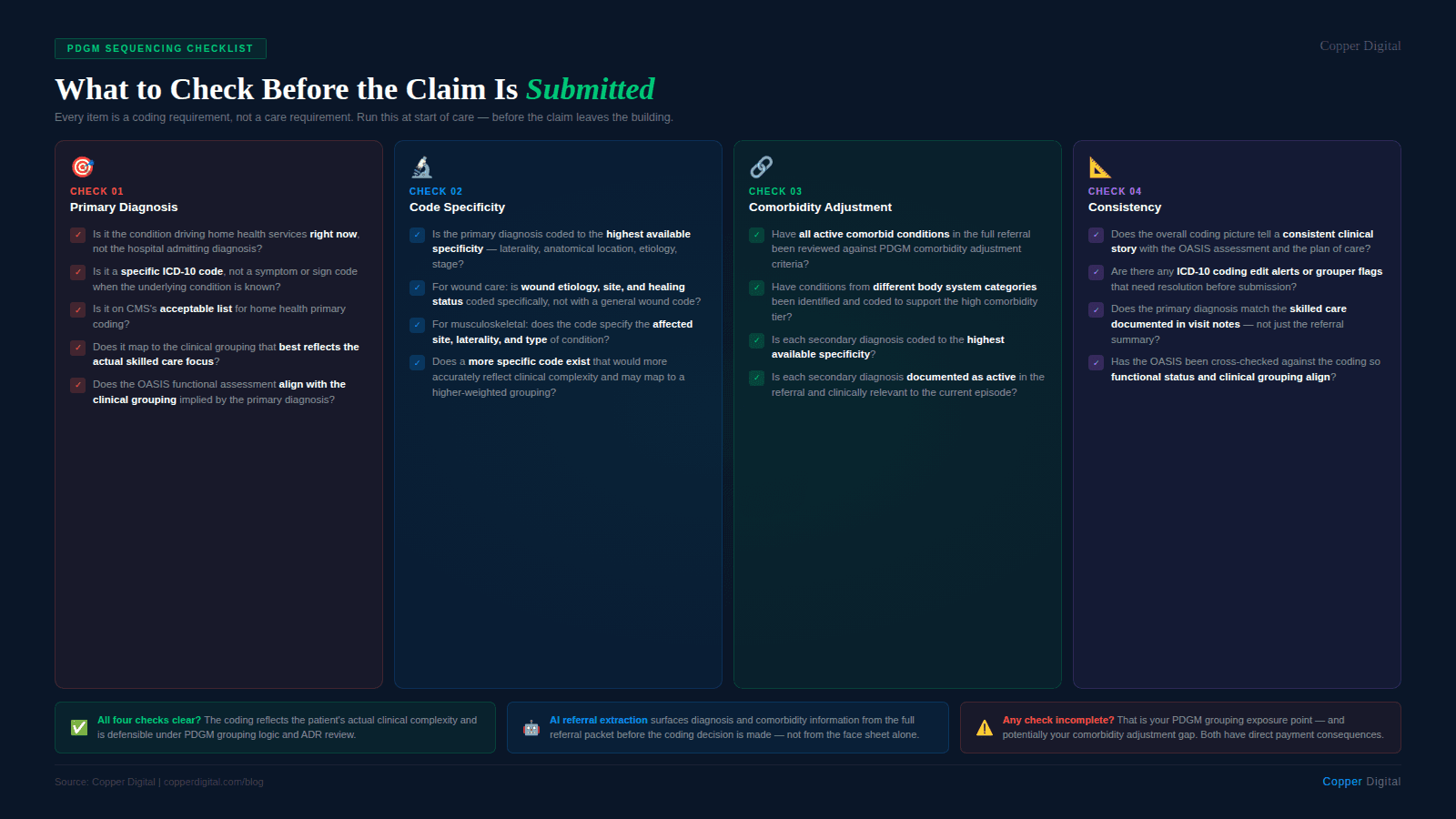
Use this checklist at start of care to evaluate the primary diagnosis selection and secondary diagnosis coding before the claim is submitted.
Primary diagnosis
Is the primary diagnosis the condition that is the primary reason for home health services during this episode, not the hospital admitting diagnosis?
Is the primary diagnosis a specific ICD-10 code, not a symptom or sign code when the underlying condition is known?
Is the primary diagnosis on CMS's acceptable list for home health primary coding?
Does the primary diagnosis map to the PDGM clinical grouping that best reflects the actual focus of skilled nursing and therapy services?
Does the OASIS functional assessment align with the clinical grouping implied by the primary diagnosis?
Specificity
Is the primary diagnosis coded to the highest available specificity, including laterality, anatomical location, etiology, and stage where applicable?
For wound care: is the wound etiology, site, and healing status coded specifically, or was a general wound code used when a more specific code is available and clinically supported?
For musculoskeletal conditions: does the code specify the affected site, laterality, and type of injury or condition?
Secondary diagnoses and comorbidity adjustment
Have all active comorbid conditions documented in the referral been reviewed against the PDGM comorbidity adjustment criteria?
Have conditions from different body system categories been coded where present, to support the high comorbidity adjustment tier?
Is each secondary diagnosis coded to the highest available specificity?
Is each secondary diagnosis documented in the referral as active and clinically relevant to the current episode?
Consistency check
Does the overall diagnosis coding picture tell a consistent clinical story with the OASIS assessment, the plan of care, and the visit note documentation?
Are there any flagged ICD-10 coding edits or grouper alerts that need to be resolved before submission?
The Revenue Impact of Getting This Right
PDGM payment differences between clinical groupings are not trivial. The base payment differential between a higher-weighted clinical grouping and a lower-weighted one can exceed several hundred dollars per 30-day payment period for the same patient. For an agency processing several hundred episodes per year, systematic sequencing errors compound into material revenue loss.
The comorbidity adjustment adds another layer. The difference between no comorbidity adjustment and a high comorbidity adjustment represents a meaningful percentage of the base payment. For a medically complex patient whose comorbidities are fully documented in the referral but only partially coded on the claim, the agency is receiving less than the reimbursement the clinical complexity warrants.
None of this involves billing for care that was not delivered. It involves coding accurately to reflect the care that was delivered and the clinical complexity of the patient who received it. The payment system is designed to adjust for complexity. Agencies that code to the full clinical picture capture the reimbursement the model intends. Agencies that code from incomplete referral extraction or misaligned sequencing leave that reimbursement uncollected.
Copper Digital extracts diagnosis and comorbidity information from referral documents at intake, surfaces it in a structured format for the coding decision, and validates primary diagnosis selection against the OASIS assessment before submission. Request a demo to see how this works in your agency's workflow. |
Related Reading

